This is an old revision of the document!
Table of Contents
Obesity Powerpoint
Obesity
Obesity is a common and preventable disease that is characterized by abnormal or excessive fat accumulation in adipose tissue.[1] The excess accumulation of fat leads to the impairment of health and is subsequently a major risk factor for the development of various non-communicable diseases such as diabetes, as well as premature death.[2]
Body Mass Index & Limitations
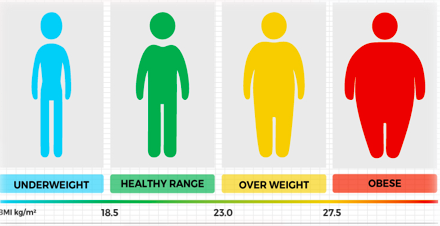
There are various methods which can be used to measure excessive adipose tissue in the body.[3] This includes skinfold thickness measurements, underwater weighing and bioelectrical impedance. The drawbacks of these methods is that they are not always readily available, the are either expensive or require highly trained personal to be conducted. In addition, many of these methods can be difficult to standardize, making it difficult for comparisons across studies and time periods.[3] Anthropometric measurements such as weight and height are the most basic methods of assessing body composition.[4] Specifically, body weight is the most frequently used measure of obesity.[4] Body mass index (BMI) is a metric that is used to assess body weight.[3] It is measured by dividing an individuals weight in kilograms by their height in meters squared. BMI is widely used as a risk factor for the development and prevalence of disease.[3]
The advantages of BMI are that it is useful for measuring obesity in a population.[4] It is a general measure of obesity that can be used for most individuals.[3] In addition, changes in BMI levels allow researchers to get a good idea of changes of obesity levels in a population.[3] Despite its strengths, BMI has many limitations when used to assess body weight.[4] For instance, it does not differentiate between lean and fat body mass. An individual may have a healthy weight according to their BMI, but still face health risks due to excessive body fat. Another limitation of BMI is that it overestimates health risks for individuals with increased muscle mass.[4]
Epidemiology
World Wide Prevalence
Undoubtedly, obesity is a disease that continues to sweep the globe. Over the past 3 and a half decades alone, the obesity prevalence has nearly doubled.5 In 2016, 650 million adults and 340 million children qualified as obese. Additionally, amongst children, 41 million under the age of 5 were considered overweight or obese.6 This constitutes a worldwide count of 990 million obese individuals. From a statistical point of view, nearly 30% of the world’s population are overweight or obese.7 Obesity tends to be more prevalent in women than in men, with 14% of women worldwide and 10% of men worldwide affected by the disease.8,9
Ethnic Prevalence
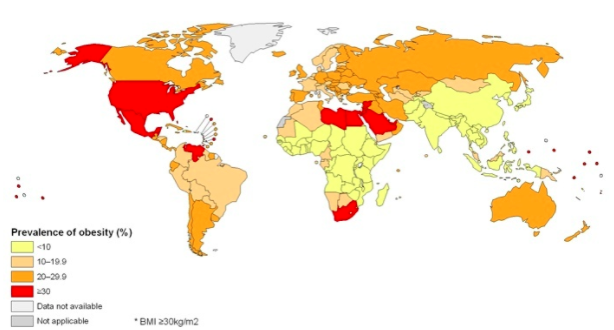
Majority of the world’s population live in countries where obesity and/or being overweight kills more people than from being underweight.6 Obesity rates are greater in certain ethnic subpopulations. The rates range from lower than 6% in Korea and Japan to greater than 30% in the United States, Mexico, New Zealand, and Hungary. Canada, Australia, United Kingdom, Chile, and South Africa are a close second, with greater than 25% of adults categorized as obese in each of these countries. In Canada, the United States, Mexico, England, France, and Switzerland, obesity rates have been on a steady incline since the 1990s. It is believed that some countries have had stabilized prevalence of obesity, however, there is no definitive indication of reduction of the epidemic anywhere.10
Canadian prevalence
In Canada, an estimated 14 million adults and 470,000 youth are characterized as obese.11 Approximately 25% of Canadians are obese. Two provinces, British Columbia and Quebec, have the lowest levels of obesity. The greatest prevalence is observed in the Northwest Territories and Newfoundland and Labrador. City-wise, the lowest levels of obesity are seen in Canada’s three largest cities: Toronto, Montreal and Vancouver.12
Ontario (local) prevalence
Ontario has been reported to have a province-wide obesity prevalence of about 25%, which is the same as the national average. However, some Ontario cities ranked in the higher end, with Sudbury, Brantford, Hamilton, and Thunder Bay being the second, fourth, fifth and seventh most obese cities, respectively, in the country.12
Evolutionary Basis of Obesity
Human babies and the need for fat
Human babies have the highest percent fat at birth for mammals.13 They have 15% body fat at birth. The second highest mammal for body fat % is the guinea pig, with 10.8. Adipose tissue is used as insulation to prevent heat from escaping the body. Human beings are hairless mammals, and therefore, are exposed to environmental stressors more directly then say a polar bear. The fur a polar bear has allows it to survive at temperatures as low as -69 degrees Celsius, even though they have a lower fat percentage than humans. Another reason humans require a high fat percentage at birth is because of the size of their brains. It is estimated that the infant brain consumes 50-60% of its total metabolic expenditure.14 The brain is not only an expensive organ, but it is also a sensitive one. It requires lots of fat to maintain itself and grow, as well as insulation to keep it at a steady temperature of around 38 degrees Celsius. This explains our natural tendency to store fat more effectively than other mammals.
An important question remains: If obesity is such a detrimental condition to the human population, then why is it so evident today?
Theory One
Evolutionarily speaking, the ability to store fat is quite the effective adaptation. Food supplies could be abundant one day, and depleted the next. This is why it is believed that another major reason for fat storage in humans is in fact an energy reserve.15 Although obesity is quite the pandemic in many developed nations today, it was rare throughout our evolutionary history within primitive populations. In fact, there is evidence to suggest no obesity within traditional hunting and gathering populations.15 Regardless, those with genes that promoted greater storage of fat had a higher likelihood to survive when resources became scarce. This has led to evolutionary pressures to select for genes doing just that. In the next section concerning gender and obesity, this is elaborated in more detail.
Theory Two
Obesity was often perceived as a status of wealth and power.15 This is because only those who had access to high energy foods on a year round basis were able to actually become overweight. This would have lead it to be a desirable trait of the opposite sex over evolutionary time.
Obesity and Gender
Obesity is seen primarily in females versus males.16 Figure 1 shows the distribution of obesity by gender for differential income as well as geographic location. It is clear that regardless of social status or ethnic location the overwhelming majority of obese and overweight individuals are in fact female.In fact, 15% body fat is average for males and 25% is average for females.16 This is the case for several reasons. Firstly, woman (evolutionarily speaking) were not required to engage in as many physically demanding activities as males were. Males, having to hunt, build etc were exposed to greater stressors on their bodies compared to their female counterparts.15 This lead to a higher percentage of muscle mass, and a lower percentage of fat for males. The second (and perhaps more pressing reason) is the fact that females are tasked with giving birth. Child bearing is very costly to a mother, and requires a large amount of energy to facilitate a very fragile fetus. Further, following childbirth breast milk is excreted that is full of nutrients and fat. This high fat milk is crucial to the development of a healthy child.17
* add graph with gender and bar graphs
Pathophysiology
Macronutrients Vs Micronutrients
Macronutrients Vs Micronutrients Macronutrients are the energy providing nutrients and are thus needed in larger amounts. These include carbohydrates, proteins and fats.18 Carbohydrates are they body’s main energy source, whereas proteins provide the amino acids important for the cell structure and the cell membrane.18 On the other hand, fats are used for making steroid and hormones in the body.18 Furthermore, fats have the highest caloric content with approximately 9 calories per gram of fat, and when burned, they provide the largest amount of energy compared to carbohydrates and proteins.18 It has been reported that a high-fat diet induces the development of obesity.19 There is a direct correlation between the amount of dietary fat and overconsumption, thus leading to weight gain.19 It is speculated that this may be due to dietary fat’s weak satiety properties, leading to the feeling of not being satisfied or full after a meal.19
Micronutrients on the other hand are needed in smaller quantities and are essential for various chemical reactions in the body.18 These include vitamins and minerals.18 Vitamins allow for normal growth and metabolism as well as cellular functions.18 These may be fat-soluble vitamins which are stored in the fatty tissues such as Vitamins A, D, E and K.18 They may also be water-soluble which are excreted in the urine and must be taken daily such as Vitamins B and C.18 Minerals are ionized in the body, for instance iron, sodium and potassium.18
Types of Adipocytes
Body fat or adipose tissue is composed of loose connective tissue which mostly consists of adipocytes or fat cells (6). White adipose tissue (WAT) and brown adipose tissue (BAT) are the two types of adipocytes which make up the majority of adipose tissue (6). Beige adipocytes are a third type of adipocyte, which have recently been identified, however their function and origin is not well understood (7).
White adipocytes are the main cell type found in human adipose tissue (6). Their main function is to store energy and they provide most of the total body fat. WAT cells have receptors for insulin, sex hormones, norepinephrine and glucocorticoids (6). They secrete proteins such as leptin, adiponectin as well as other adipokines (7). Furthermore, WAT is involved in controlling metabolism by acting as a thermal insulator to help maintain energy homeostasis (7).
Brown adipocytes are found in almost in all mammals and they function to dissipate energy through thermogenesis (8). Their characteristic brown appearance is due to a high number of iron-containing mitochondria (8). BAT develop from the middle embryonic layer, the mesoderm, which is also the source of muscle cells and adipocytes (6). It is abundant in newborns as well as metabolically active adult humans, however, its prevalence decreases in humans as they age (6). Furthermore, brown adipocytes also contain more capillaries than white fat, which allows for tissue to be supplied with more oxygen and nutrients (8). In this way, produced heat can easily be distributed throughout the body (8).
*insert adipose figure 4 image
Normal Function of Adipose Tissue & Adipose Tissue Development
Adipose tissue is an endocrine organ which is mainly responsible for energy storage as well as the synthesis and secretion of several hormones (9)20. Adipose tissue is a major source of free fatty acids. Free fatty acids (FFA) are liberated from lipoproteins by lipoprotein lipase, allowing it to enter the adipocyte where it is reassembled into triglycerides by esterifying it onto glycerol. Adipocytes have an important physiological role in maintaining triglyceride and FFA levels (9)20.
In conditions of obesity, hyperplasia and hypertrophy lead to the expansion of adipose tissue, which results in the development of adipocytes that are metabolically unhealthy (10).21 The activation of biological pathways that favour the differentiation of adipocytes as well as the formation of adipocytes from precursor cells produces an increase in the number of adipocytes (10). There are certain proteins and transcriptional factors involved in inhibiting or promoting the development of adipocytes (9). Adipogenesis, the development of adipose tissue, involves the differentiation of preadipocytes into mature fat cells. Changes in transcription factor expression and activity is what results in the differentiation of these pre-adipocytes into mature fat cells.Transcription factors involved in promoting adipogenesis include the AP-1 family, PPARy, STATs, members of the KLF family, SREBP-1 and members C/EBP family. Conversely, Pref-1, GATA and Wnt family transcription factors are involved in inhibiting adipogenesis (9).
Pre-adipocytes within adipose tissue can differentiate into mature adipocytes throughout their lifetime (10).This allows for the expansion of adipose tissue when increased storage requirements are needed. Furthermore, mature adipocytes have the ability to accommodate increased storage needs, and in cases of overnutrition, these cells can become hypertrophic (10).
Adipose tissue undergoes a continuous process of remodelling(11). This normally maintains tissue health, however, this process is accelerated in obesity which can lead to the death of adipocytes along with the recruitment and activation of immune cells. Increased activation of the immune system leads to inflammation, which is the hallmark of obesity. Overall, an increase in the death of adipocytes, coupled with an increase in immune cell activation leads to many of the pathophysiological consequences of obesity (11).
===== Hormones =====
Endorphin release when you eat
Some people eat more than usual when they are bored, angry, or stressed. Over time, overeating will lead to weight gain and may cause overweight or obesity [7].
Smoking
It is not uncommon to see people gain weight when they stop smoking. Nicotine raises the rate at which the body burns calories, therefore less calories are burned when one ceases from smoking [12].
Age
As we age, muscle is lost, especially if one is less active. Muscle loss can slow down the rate at which the body burns calories. Midlife weight gain in women is mainly due to aging and lifestyle, but menopause also plays a role. Many women gain about 5 pounds during menopause and have more fat around the waist than before [13].
Pregnancy
Women gain weight to support their child’s development. After giving birth, some women find it hard to lose the weight. This may lead to overweight or obesity, especially after a few pregnancies [14].
Lack of Sleep
Lack of sleep increases the risk of obesity. People who sleep fewer hours also seem to prefer eating foods that are higher in calories and carbohydrates, which can lead to overeating, weight gain, and obesity. Additionally, sleep helps maintain a healthy balance of the hormones that make you feel hungry or full. Sleep also affects how the body reacts to insulin, the hormone that controls your blood glucose level. Lack of sleep results in a higher than normal blood sugar level, which may increase the risk for diabetes [15].
===== Pathophysiology =====
==== Adipocyte Development and Metabolism ====
Obesity can be characterized by the excessive accumulation of adipocyte cells forming deposits of adipose tissue. Individuals with a healthy metabolic activity and a normal BMI undergo the process of lipolysis, which is the breakdown of lipids. Lipolysis is regulated in the process of 𝜷₁ and 𝜷₂ adrenergic receptors (ARs) signalling cyclic adenosine monophosphate (cAMP) dependent protein kinase to initiate the phosphorylation of perilipin and hormone-sensitive lipase. Adipocytes express elevated levels of α₂ adrenergic receptors, which inhibit the expression of cAMP, thus preventing lipolysis. Furthermore, reduced lipolytic regulation is evident in hypertrophic subcutaneous fat cells, as they contain more α₂ ARs in comparison to 𝜷₁ and 𝜷₂ ARs. Defects or polymorphisms in the 𝜷₂ AR gene may also impede in the process of lipid breakdown [16].
In events of inadequate caloric intake, adipocytes allow excess energy to be stored as triacylglycerol. Non-esterified fatty acids (NEFAs) are primarily involved in insulin signalling, however they are also released when triacylglycerol stores undergo lipolysis. While triacylglycerol synthesis and lipolysis occur in a balanced manner under normal conditions, NEFAs are increased in obese individuals, thus posing a risk for Type 2 diabetes [16].
The secretory activity of adipocytes plays a huge role in regards to hormonal and metabolic activity that takes place. Adipose cells are increased in size and number in obese conditions, which initiate an immune response. The fat cells release pro-inflammatory adipokines that recruit macrophages to the site. Following this, Tumour Necrosis Factor- alpha (TNF-α) is released and additional immune cells are brought to the site. This constant state of inflammation causes insulin resistance. This is why diabetes is often comorbid with obesity [17]. This sequence of events is depicted in Figure 7.
<box 35% round left |> </box|Figure 7:This figure is a visual depiction of the secretory pathway and function of adipokines in conditions where excessive adipocyte buildup occurs from http://www.the-scientist.com/images/December2012/Obese_Infograph.jpg>
When analyzing other inflammatory factors, it is evident that increased concentrations of the adipokine Interleukin-6 (IL-6) are positively correlated with increased fat mass and BMI. Furthermore, IL-6 is increases post-exercise with increased NEFAs, thus proposing a correlation between the adipokine and lipid mobilization [16].Monophosphate activated protein kinase (AMPK) enables the oxidation of fatty acids during muscle contraction. AMPK is regulated by the hormone adiponectin, which induces insulin-sensitivity. In individuals who are obese, the concentration of adiponectin is reduced, as individuals with symptoms of diabetes are resistant to insulin [16].
==== Hormone Regulation ====
The hormonal regulation of insulin, leptin and ghrelin is affected in obese individuals. Hormonal imbalances cause physiological changes that impede on appetite suppression and insulin sensitivity. Figure 8 shows human hormones and food intake.
Insulin
Insulin is a hormone secreted by the 𝜷 cells in the pancreas [18].
They regulate glucose levels by storing glucose into muscle, fat, and liver cells. In obese individuals, we see a high incidence of insulin resistance, therefore insulin is unable to regulate glucose levels. Under normal physiological conditions, food is broken down into glucose post-consumption, and the pancreas secretes appropriate levels of insulin to maintain homeostatic levels of plasma glucose. Due to the fact that insulin displays insensitivity in obese individuals, the glucose absorbance is very low. Since the cells do not have energy, appetite-suppression is hindered and overeating occurs. The detrimental effects of this include an excessive blood glucose and insulin release, thus making obese individuals more susceptible to Type 2 diabetes. [18].
Investigating the molecular mechanism underlying insulin resistance is important towards understanding the relationship between insulin and obesity. There are many mechanisms through which insulin is able to promote the accumulation of fat in adipocytes, such as the early differentiation of preadipocytes to mature adipocytes, the unregulated transportation of glucose, the upregulation of lipogenesis, and the downregulation of lipolysis[19].
Leptin
Leptin is an appetite-suppressing peptide hormone that is secreted by adipocytes[20]. In obese individuals, there is a greater mass of adipose tissue, which directly correlates with a greater secretion of leptin. Theoretically, when there is more leptin, individuals should consume less, because the hormone is appetite suppressing. However, there is a higher appetite-stimulating effect in obese individuals. This suggests that individuals who are obese display leptin resistance.
A study conducted by Kazmi et al.(1996) investigated leptin concentrations in a sample of a Rawalpindi population. There were three sampling groups—health obese, overweight and non-obese. According to the results, the mean serum leptin concentration for the obese group was 52.8 ug/mL and 6.3 ug/mL for the non-obese group. The results of this study concluded there is certainly a positive correlation between the Body Mass Index and leptin concentrations in individuals [21].
<box 45% round right|>
</box|Figure 7:This figure is a visual depiction of the secretory pathway and function of adipokines in conditions where excessive adipocyte buildup occurs from http://www.the-scientist.com/images/December2012/Obese_Infograph.jpg>
When analyzing other inflammatory factors, it is evident that increased concentrations of the adipokine Interleukin-6 (IL-6) are positively correlated with increased fat mass and BMI. Furthermore, IL-6 is increases post-exercise with increased NEFAs, thus proposing a correlation between the adipokine and lipid mobilization [16].Monophosphate activated protein kinase (AMPK) enables the oxidation of fatty acids during muscle contraction. AMPK is regulated by the hormone adiponectin, which induces insulin-sensitivity. In individuals who are obese, the concentration of adiponectin is reduced, as individuals with symptoms of diabetes are resistant to insulin [16].
==== Hormone Regulation ====
The hormonal regulation of insulin, leptin and ghrelin is affected in obese individuals. Hormonal imbalances cause physiological changes that impede on appetite suppression and insulin sensitivity. Figure 8 shows human hormones and food intake.
Insulin
Insulin is a hormone secreted by the 𝜷 cells in the pancreas [18].
They regulate glucose levels by storing glucose into muscle, fat, and liver cells. In obese individuals, we see a high incidence of insulin resistance, therefore insulin is unable to regulate glucose levels. Under normal physiological conditions, food is broken down into glucose post-consumption, and the pancreas secretes appropriate levels of insulin to maintain homeostatic levels of plasma glucose. Due to the fact that insulin displays insensitivity in obese individuals, the glucose absorbance is very low. Since the cells do not have energy, appetite-suppression is hindered and overeating occurs. The detrimental effects of this include an excessive blood glucose and insulin release, thus making obese individuals more susceptible to Type 2 diabetes. [18].
Investigating the molecular mechanism underlying insulin resistance is important towards understanding the relationship between insulin and obesity. There are many mechanisms through which insulin is able to promote the accumulation of fat in adipocytes, such as the early differentiation of preadipocytes to mature adipocytes, the unregulated transportation of glucose, the upregulation of lipogenesis, and the downregulation of lipolysis[19].
Leptin
Leptin is an appetite-suppressing peptide hormone that is secreted by adipocytes[20]. In obese individuals, there is a greater mass of adipose tissue, which directly correlates with a greater secretion of leptin. Theoretically, when there is more leptin, individuals should consume less, because the hormone is appetite suppressing. However, there is a higher appetite-stimulating effect in obese individuals. This suggests that individuals who are obese display leptin resistance.
A study conducted by Kazmi et al.(1996) investigated leptin concentrations in a sample of a Rawalpindi population. There were three sampling groups—health obese, overweight and non-obese. According to the results, the mean serum leptin concentration for the obese group was 52.8 ug/mL and 6.3 ug/mL for the non-obese group. The results of this study concluded there is certainly a positive correlation between the Body Mass Index and leptin concentrations in individuals [21].
<box 45% round right|> </box|Figure 8: Human hormones and food intake from http://blog.naturessunshine.com/wp-content/uploads/2015/12/Control_Food_Intake.jpg>
Ghrelin
Ghrelin is an appetite-stimulating hormone secreted primarily by the stomach during times of low caloric intake [20]. It signals individuals to increase their food intake and promote fat storage. The concentration of ghrelin is expected to be higher with obesity, because it would account for the increased food intake in cases of obesity. However, experimental evidence shows that Ghrelin concentrations are actually much lower in obese individuals. To investigate the role of ghrelin in obese pathology, Tschop et al. (2001) conducted a study where the plasma ghrelin concentrations of lean and obese individuals were measured. The plasma ghrelin concentrations of obese individuals were much lower than in lean individuals [22]. There seemed to be a negative correlation between plasma ghrelin concentrations and fat mass.
The body’s instinctive shift for homeostasis could account for the downregulation of plasma ghrelin in obese individuals. Since ghrelin and leptin display antagonistic properties, it would not be possible for there to be high concentrations of both hormones. High leptin concentrations could account for low concentrations of ghrelin [20]. The exact mechanism through which this happens is yet to be elucidated by research.
==== Genetic Predisposition ====
When assessing the heritability of obesity, it has a numerical association of 0.7, which is fairly high relative to heritability in schizophrenia (0.81) and autism (0.9). In the case of rare familial obesity, gene defects occur in appetite regulation. Variants in the leptin-melanocortin pathway result in about 5% of morbid human obesity. Common polygenic obesity is characterized by the human obesity gene map. When performing a closer analysis of some of the key factors involved in obesity, Pre-B cell colony enhancing factor (PBEF1), which is secreted by lymphocytes, is expressed by adipocytes. Presently, it is referred to as Visfatin [23].
Due to the interconnectedness of genes, it can be difficult to address conflicting effects of similar genetic factors. Ghrelin binds to the growth hormone secretagogue receptor (GHSR), and initially, variants of GHSR were evident in common obesity and rare familial obesity. More recent studies show a negative correlation between GHSR variants and obesity. It is hypothesized that these effects could be due to obestatin, which is a hormone that regulates appetite in the opposite way that ghrelin does [23].
Having the ability to detect the genetic basis for obesity provides therapeutic solutions that can combat symptoms of obesity. A variety of biomarkers have been identified as factors involved in obesity. These biomarkers are used to differentiate between types of obesity, provide insight on the associated comorbid diseases, genetic susceptibility and explain the implications of the interaction between two or more factors [23].
Areas of research pertaining to molecular genetics are expanding the scope of genetic predispositions involved in obesity. As of October 2005, 244 mutated genes or transgenes causing phenotypic changes in weight and adiposity are identified. The human obesity gene map indicates that 176 human obesity cases can be linked to 11 specific genes, and 50 loci pertaining to human obesity are linked to Mendelian syndromes [24]
The gene map (Figure 9), includes all obesity-related genes and quantitative trait loci identified from the various lines of evidence reviewed in the paper. It is further explained and categorized into the 5 categories, where information pertaining to the mouse chromosome, mouse gene, human chromosome, human homolog, statistical analyses of variance, gene description, details pertaining to its role in obesity and more is provided. Areas of research pertaining to molecular genetics are expanding the scope of genetic predispositions involved in obesity [24].
</box|Figure 8: Human hormones and food intake from http://blog.naturessunshine.com/wp-content/uploads/2015/12/Control_Food_Intake.jpg>
Ghrelin
Ghrelin is an appetite-stimulating hormone secreted primarily by the stomach during times of low caloric intake [20]. It signals individuals to increase their food intake and promote fat storage. The concentration of ghrelin is expected to be higher with obesity, because it would account for the increased food intake in cases of obesity. However, experimental evidence shows that Ghrelin concentrations are actually much lower in obese individuals. To investigate the role of ghrelin in obese pathology, Tschop et al. (2001) conducted a study where the plasma ghrelin concentrations of lean and obese individuals were measured. The plasma ghrelin concentrations of obese individuals were much lower than in lean individuals [22]. There seemed to be a negative correlation between plasma ghrelin concentrations and fat mass.
The body’s instinctive shift for homeostasis could account for the downregulation of plasma ghrelin in obese individuals. Since ghrelin and leptin display antagonistic properties, it would not be possible for there to be high concentrations of both hormones. High leptin concentrations could account for low concentrations of ghrelin [20]. The exact mechanism through which this happens is yet to be elucidated by research.
==== Genetic Predisposition ====
When assessing the heritability of obesity, it has a numerical association of 0.7, which is fairly high relative to heritability in schizophrenia (0.81) and autism (0.9). In the case of rare familial obesity, gene defects occur in appetite regulation. Variants in the leptin-melanocortin pathway result in about 5% of morbid human obesity. Common polygenic obesity is characterized by the human obesity gene map. When performing a closer analysis of some of the key factors involved in obesity, Pre-B cell colony enhancing factor (PBEF1), which is secreted by lymphocytes, is expressed by adipocytes. Presently, it is referred to as Visfatin [23].
Due to the interconnectedness of genes, it can be difficult to address conflicting effects of similar genetic factors. Ghrelin binds to the growth hormone secretagogue receptor (GHSR), and initially, variants of GHSR were evident in common obesity and rare familial obesity. More recent studies show a negative correlation between GHSR variants and obesity. It is hypothesized that these effects could be due to obestatin, which is a hormone that regulates appetite in the opposite way that ghrelin does [23].
Having the ability to detect the genetic basis for obesity provides therapeutic solutions that can combat symptoms of obesity. A variety of biomarkers have been identified as factors involved in obesity. These biomarkers are used to differentiate between types of obesity, provide insight on the associated comorbid diseases, genetic susceptibility and explain the implications of the interaction between two or more factors [23].
Areas of research pertaining to molecular genetics are expanding the scope of genetic predispositions involved in obesity. As of October 2005, 244 mutated genes or transgenes causing phenotypic changes in weight and adiposity are identified. The human obesity gene map indicates that 176 human obesity cases can be linked to 11 specific genes, and 50 loci pertaining to human obesity are linked to Mendelian syndromes [24]
The gene map (Figure 9), includes all obesity-related genes and quantitative trait loci identified from the various lines of evidence reviewed in the paper. It is further explained and categorized into the 5 categories, where information pertaining to the mouse chromosome, mouse gene, human chromosome, human homolog, statistical analyses of variance, gene description, details pertaining to its role in obesity and more is provided. Areas of research pertaining to molecular genetics are expanding the scope of genetic predispositions involved in obesity [24].
 Figure 9: Human obesity gene map, updated in 2005.
From http://onlinelibrary.wiley.com.libaccess.lib.mcmaster.ca/doi/10.1038/oby.2006.71/full
===== Treatments =====
Goals of Weight Loss and Management
When undergoing weight loss therapy, practice guidelines issued by the National Heart, Lung and Blood Institute and the North American Association for the Study of Obesity recommend an initial weight loss goal of approximately 10% from baseline over a period of 6 months of therapy [25].
A weight loss of 10% has the potential to improve glycemic control, blood pressure control and lipid levels, especially in individuals with Type 2 diabetes or hypertension. Additionally, it might help to reduce symptoms from comorbidities, such as gastroesophageal reflux and osteoarthritis. If weight loss is maintained over a long period of time, adverse clinical outcomes, such as myocardial infarction, stroke and cardiovascular-related deaths, can be reduced [26].
Intervention
For the optimal weight loss and health benefits, it is important to adopt lifestyle modifications, such as dietary therapy, physical activity and cognitive behaviour therapy. Typically, health care practitioners recommend their patients to pursue the lifestyle modifications for 6 months. Thereafter, clinicians assess whether they have reached the weight loss goal of 10% from baseline estimates. If patients have attained a satisfactory progression upon evaluation, it is recommended that they maintain their lifestyle modifications for sustainable weight loss results. Regular monitoring is a crucial aspect of ensuring a healthy lifestyle, as the influences of side effects must also be considered. In the case that patients have not attained their recommended weight after 6 months, health care practitioners typically recommend pharmacotherapy and/ or bariatric surgery to achieve their weight loss goal. The most conclusive results are seen when either pharmacotherapy or bariatric surgery are used in conjunction with lifestyle modifications [25].
Diet
<box 25% round right |>
Figure 9: Human obesity gene map, updated in 2005.
From http://onlinelibrary.wiley.com.libaccess.lib.mcmaster.ca/doi/10.1038/oby.2006.71/full
===== Treatments =====
Goals of Weight Loss and Management
When undergoing weight loss therapy, practice guidelines issued by the National Heart, Lung and Blood Institute and the North American Association for the Study of Obesity recommend an initial weight loss goal of approximately 10% from baseline over a period of 6 months of therapy [25].
A weight loss of 10% has the potential to improve glycemic control, blood pressure control and lipid levels, especially in individuals with Type 2 diabetes or hypertension. Additionally, it might help to reduce symptoms from comorbidities, such as gastroesophageal reflux and osteoarthritis. If weight loss is maintained over a long period of time, adverse clinical outcomes, such as myocardial infarction, stroke and cardiovascular-related deaths, can be reduced [26].
Intervention
For the optimal weight loss and health benefits, it is important to adopt lifestyle modifications, such as dietary therapy, physical activity and cognitive behaviour therapy. Typically, health care practitioners recommend their patients to pursue the lifestyle modifications for 6 months. Thereafter, clinicians assess whether they have reached the weight loss goal of 10% from baseline estimates. If patients have attained a satisfactory progression upon evaluation, it is recommended that they maintain their lifestyle modifications for sustainable weight loss results. Regular monitoring is a crucial aspect of ensuring a healthy lifestyle, as the influences of side effects must also be considered. In the case that patients have not attained their recommended weight after 6 months, health care practitioners typically recommend pharmacotherapy and/ or bariatric surgery to achieve their weight loss goal. The most conclusive results are seen when either pharmacotherapy or bariatric surgery are used in conjunction with lifestyle modifications [25].
Diet
<box 25% round right |> </box|Figure 10: Illustration of the ideal food plate including all food groups from http://www.arthritis.org/images/slideshows/ra-diet/ra-diet-13-fill-your-plate.jpg
>
The first component of lifestyle modifications to treating obesity is undergoing dietary therapy (Figure 10). When assessing diet management in obese patients, weight reduction is highly dependent upon energy intake in comparison to energy expenditure [27].
According to a study conducted by Poirier and Despres (2001), it has been concluded that approximately 1 pound of mass can be lost within a week without any changes being made to the level of physical activity [27]. There are various types of diets that an individual can choose to pursue. Each type of diet is subjective to the patient, therefore it can produce differing results. Three diets that are typically suggested to obese patients are the low carbohydrate diet, the low-fat diet and the high protein diet.
The low carbohydrate diet is consists of a reduced carbohydrate consumption [28]. Long-term studies have shown that low carbohydrate diets produce significant results at the 3 and 6 month points. However, results become insignificant at about a year onwards [29]. When examining the weight reduction that high protein diets produced, the results were indifferent [29]. Patients were losing a significant amount of weight up until about a year and then the results started to decrease [29]. Studies about the low-fat diet have shown that patients saw a significant weight reduction for about three years and then results were insignificant [30].
Although all three of these diets show promising results, the low carbohydrate and high protein diets show short term effects, while the low fat diet seems to display long term fat reduction. In conclusion, it is important to note that many individuals are susceptible to regaining their weight, thus a sustainable lifestyle is integral. Managing weight loss through dietary means can be difficult, however it can be made easier when incorporating physical activity into the daily routine.
Weight Loss Programs
Due to the vast technological advances of our time, there are many weight loss programs available that are highly accessible. Although there are a wide variety of programs to choose from, it is always encouraged to keep in mind that not every weight loss program will produce the same kinds of results for everyone. It is always important to consult with a family physician when trying to find a weight loss program that will have a positive effect on a personal weight reduction.
Some examples of weight loss programs that are available for further investigation are listed below:
The Paleo Diet: It works to incorporate whole foods, lean protein, veggies, fruits, nuts, and seeds and encourages to stay away from foods with sugars, dairy and grains.
The Vegan Diet: It is an ‘extreme’ vegetarian diet that works to eliminate dairy, eggs, and animal derived products, such as gelatin, honey, whey, and vitamin D3.
The Low Carbohydrate Diet: It encourages individuals to eat an unlimited amount of protein and fat, while completely eliminating carbohydrates.
The Ultra Low-Fat Diet: It consists of a diet where 10% or less calories come from fat. This diet is almost entirely made up plant based food items, with a very limited intake of animal products.
The Zone Diet: This diet encourages participants to balance each meal with one third of protein, and two thirds of fruits and veggies. A small amount of fat that comes from natural and healthy sources, such as avocado, almonds, or olive oil can also be consumed.
Intermediate Fasting: This diet challenges its participants to fast during portions of the day, while restricting the calorie intake during the times you do choose to eat. This diet is most efficient when you aren’t overeating during the times where the fast has been broken.
There are a few options when trying to reduce weight loss. All of the diets that are listed above prove to have a positive impact on weight reduction. However every diet has its consequences. When the body is restricted from having certain kinds of foods, nutrients, minerals and vitamins are compromised. For example, if an individual were to go on the paleo diet, the restriction of whole grains and dairy prevents individuals from consuming certain vitamins. A family physician or a dietician would be able to provide the most representative diet plan for each individual [31].
Physical Activity
The second component of the lifestyle modifications approach to treating obesity is to be physically active. The purpose behind weight loss and management programs is to stop future weight gain, decrease body weight and permanently maintain a lower body weight [32]. Maintaining a physically active lifestyle is known to be key to a long term weight maintenance, because it increases the energy expenditure through caloric deficit [33]. When incorporating physical activity into a daily routine with hopes of maintaining the reduction of body weight, it is important to remember that different training modalities such as walking, cycling and swimming can have a different impact on different individuals [34].
When involved in physical activity, many adaptive responses take place, which cause a more efficient system for oxygen transfer to muscle [32]. In addition, reduced adipose tissue mass representing an important mechanical advantage, allows better long-term work [32]. Physical training helps counteract the permissive and affluent environment that predisposes reduced-obese subjects to regain weight [32]. Many studies have recommended thirty to forty-five minutes of moderately intensive physical activity, to be done 3-5 times a week [35]. In particular, public health interventions have promoted walking as a physical activity, since it is safe, accessible and a low intense aerobic exercise that results in high fat loss [32]. Losing weight through physical activity can be very difficult, especially for obese patients and therefore, it is important to set realistic weight loss goals of about 0.5-1 pound per week, with the assistance [32]. Because it may seem like small steps are made in weight reduction while working out, it is important for patients to remain determined and persevere to reach their goals [32]. Keeping a positive attitude during this process can be very difficult and so, it is extremely important for the patient to have one-on-one interaction between the clinician or healthcare professional on a regular basis [32].
Cognitive Behaviour Therapy
<box 30% round right |>
</box|Figure 10: Illustration of the ideal food plate including all food groups from http://www.arthritis.org/images/slideshows/ra-diet/ra-diet-13-fill-your-plate.jpg
>
The first component of lifestyle modifications to treating obesity is undergoing dietary therapy (Figure 10). When assessing diet management in obese patients, weight reduction is highly dependent upon energy intake in comparison to energy expenditure [27].
According to a study conducted by Poirier and Despres (2001), it has been concluded that approximately 1 pound of mass can be lost within a week without any changes being made to the level of physical activity [27]. There are various types of diets that an individual can choose to pursue. Each type of diet is subjective to the patient, therefore it can produce differing results. Three diets that are typically suggested to obese patients are the low carbohydrate diet, the low-fat diet and the high protein diet.
The low carbohydrate diet is consists of a reduced carbohydrate consumption [28]. Long-term studies have shown that low carbohydrate diets produce significant results at the 3 and 6 month points. However, results become insignificant at about a year onwards [29]. When examining the weight reduction that high protein diets produced, the results were indifferent [29]. Patients were losing a significant amount of weight up until about a year and then the results started to decrease [29]. Studies about the low-fat diet have shown that patients saw a significant weight reduction for about three years and then results were insignificant [30].
Although all three of these diets show promising results, the low carbohydrate and high protein diets show short term effects, while the low fat diet seems to display long term fat reduction. In conclusion, it is important to note that many individuals are susceptible to regaining their weight, thus a sustainable lifestyle is integral. Managing weight loss through dietary means can be difficult, however it can be made easier when incorporating physical activity into the daily routine.
Weight Loss Programs
Due to the vast technological advances of our time, there are many weight loss programs available that are highly accessible. Although there are a wide variety of programs to choose from, it is always encouraged to keep in mind that not every weight loss program will produce the same kinds of results for everyone. It is always important to consult with a family physician when trying to find a weight loss program that will have a positive effect on a personal weight reduction.
Some examples of weight loss programs that are available for further investigation are listed below:
The Paleo Diet: It works to incorporate whole foods, lean protein, veggies, fruits, nuts, and seeds and encourages to stay away from foods with sugars, dairy and grains.
The Vegan Diet: It is an ‘extreme’ vegetarian diet that works to eliminate dairy, eggs, and animal derived products, such as gelatin, honey, whey, and vitamin D3.
The Low Carbohydrate Diet: It encourages individuals to eat an unlimited amount of protein and fat, while completely eliminating carbohydrates.
The Ultra Low-Fat Diet: It consists of a diet where 10% or less calories come from fat. This diet is almost entirely made up plant based food items, with a very limited intake of animal products.
The Zone Diet: This diet encourages participants to balance each meal with one third of protein, and two thirds of fruits and veggies. A small amount of fat that comes from natural and healthy sources, such as avocado, almonds, or olive oil can also be consumed.
Intermediate Fasting: This diet challenges its participants to fast during portions of the day, while restricting the calorie intake during the times you do choose to eat. This diet is most efficient when you aren’t overeating during the times where the fast has been broken.
There are a few options when trying to reduce weight loss. All of the diets that are listed above prove to have a positive impact on weight reduction. However every diet has its consequences. When the body is restricted from having certain kinds of foods, nutrients, minerals and vitamins are compromised. For example, if an individual were to go on the paleo diet, the restriction of whole grains and dairy prevents individuals from consuming certain vitamins. A family physician or a dietician would be able to provide the most representative diet plan for each individual [31].
Physical Activity
The second component of the lifestyle modifications approach to treating obesity is to be physically active. The purpose behind weight loss and management programs is to stop future weight gain, decrease body weight and permanently maintain a lower body weight [32]. Maintaining a physically active lifestyle is known to be key to a long term weight maintenance, because it increases the energy expenditure through caloric deficit [33]. When incorporating physical activity into a daily routine with hopes of maintaining the reduction of body weight, it is important to remember that different training modalities such as walking, cycling and swimming can have a different impact on different individuals [34].
When involved in physical activity, many adaptive responses take place, which cause a more efficient system for oxygen transfer to muscle [32]. In addition, reduced adipose tissue mass representing an important mechanical advantage, allows better long-term work [32]. Physical training helps counteract the permissive and affluent environment that predisposes reduced-obese subjects to regain weight [32]. Many studies have recommended thirty to forty-five minutes of moderately intensive physical activity, to be done 3-5 times a week [35]. In particular, public health interventions have promoted walking as a physical activity, since it is safe, accessible and a low intense aerobic exercise that results in high fat loss [32]. Losing weight through physical activity can be very difficult, especially for obese patients and therefore, it is important to set realistic weight loss goals of about 0.5-1 pound per week, with the assistance [32]. Because it may seem like small steps are made in weight reduction while working out, it is important for patients to remain determined and persevere to reach their goals [32]. Keeping a positive attitude during this process can be very difficult and so, it is extremely important for the patient to have one-on-one interaction between the clinician or healthcare professional on a regular basis [32].
Cognitive Behaviour Therapy
<box 30% round right |> </box|Figure 11: The three main components of Cognitive Behaviour Therapy: thought, emotion and behaviour
from http://in8.uk.com/wp-content/uploads/2016/03/CBT-image.png>
The third component of lifestyle modifications is to undergo cognitive behaviour therapy (CBT) to assess one’s current habits and identify factors, stressors or situations that may trigger one’s overeating habits and contribute to their obesity (Figure 11). With a CBT approach, patients suffering from obesity can get help through counseling, support groups, as well as adopt the family-based approach [25,26].
The purpose of the CBT treatment is not to eliminate a psychiatric disorder but to change eating and exercise behaviours [36]. This intervention aims to educate individuals on how to change problematic behaviours. Firstly, CBT is based on the cognitive conceptualization of the processes that lead to overeating. Specifically, thoughts and thinking patterns that are considered central to the problem. Secondly, CBT is focused on altering the cognitive and behavioural mechanisms that maintain the problem behaviour. Lastly, CBT uses both cognitive and behavioural techniques to maintain healthy mechanisms [37]. The diagram here shows different components that contribute to CBT.
Counselling is one way a patient can undergo CBT. It can either be delivered on a one-on-one basis, or in a group setting of approximately 10 participants with a trained healthcare professional [38,39]. A study conducted by Renjilian and colleagues comparing the two treatment modalities concluded that participants who were randomized to receive group-based therapy lost more weight after 26 weekly sessions compared to those who were treated individually. Specifically, those receiving group therapy lost about 11 kg after 26 weekly sessions, in comparison to 9 kg for those who were individually treated [40].
In addition to counselling, having a support network is important. This is especially true if the individual is undergoing drastic changes. Receiving encouragement from family, friends and health care practitioners can be very motivating during challenging times of the weight loss and maintenance programs. Furthermore, patients can also join support groups with other people undergoing weight loss [25].
Family-based obesity treatment has also been proven to be a very effective and sustainable approach, especially when treating pediatric obesity. The role of this treatment is to target eating and activity change in both child and parent. Programs using this approach teach parents behavioural skills to facilitate child behaviour change and utilize family resources to improve the efficacy of childhood obesity treatments. Simultaneously treating the child and parent helps create positive relationships between them as they both aim to reach their weight loss goal together [41,42].
Pharmacotherapy
The Canadian Clinical Practice Guidelines on the Management and Prevention of Obesity in Adults and Children recommends that in addition to lifestyle modifications such as dietary changes, physical activity and behaviour therapy, overweight individuals with BMIs greater than 27 kg/m^2 but with life threatening diseases, or obese individuals with BMIs greater than 30 kg/m^2 can undergo pharmacotherapy [2].
<box 35% round right |>
</box|Figure 11: The three main components of Cognitive Behaviour Therapy: thought, emotion and behaviour
from http://in8.uk.com/wp-content/uploads/2016/03/CBT-image.png>
The third component of lifestyle modifications is to undergo cognitive behaviour therapy (CBT) to assess one’s current habits and identify factors, stressors or situations that may trigger one’s overeating habits and contribute to their obesity (Figure 11). With a CBT approach, patients suffering from obesity can get help through counseling, support groups, as well as adopt the family-based approach [25,26].
The purpose of the CBT treatment is not to eliminate a psychiatric disorder but to change eating and exercise behaviours [36]. This intervention aims to educate individuals on how to change problematic behaviours. Firstly, CBT is based on the cognitive conceptualization of the processes that lead to overeating. Specifically, thoughts and thinking patterns that are considered central to the problem. Secondly, CBT is focused on altering the cognitive and behavioural mechanisms that maintain the problem behaviour. Lastly, CBT uses both cognitive and behavioural techniques to maintain healthy mechanisms [37]. The diagram here shows different components that contribute to CBT.
Counselling is one way a patient can undergo CBT. It can either be delivered on a one-on-one basis, or in a group setting of approximately 10 participants with a trained healthcare professional [38,39]. A study conducted by Renjilian and colleagues comparing the two treatment modalities concluded that participants who were randomized to receive group-based therapy lost more weight after 26 weekly sessions compared to those who were treated individually. Specifically, those receiving group therapy lost about 11 kg after 26 weekly sessions, in comparison to 9 kg for those who were individually treated [40].
In addition to counselling, having a support network is important. This is especially true if the individual is undergoing drastic changes. Receiving encouragement from family, friends and health care practitioners can be very motivating during challenging times of the weight loss and maintenance programs. Furthermore, patients can also join support groups with other people undergoing weight loss [25].
Family-based obesity treatment has also been proven to be a very effective and sustainable approach, especially when treating pediatric obesity. The role of this treatment is to target eating and activity change in both child and parent. Programs using this approach teach parents behavioural skills to facilitate child behaviour change and utilize family resources to improve the efficacy of childhood obesity treatments. Simultaneously treating the child and parent helps create positive relationships between them as they both aim to reach their weight loss goal together [41,42].
Pharmacotherapy
The Canadian Clinical Practice Guidelines on the Management and Prevention of Obesity in Adults and Children recommends that in addition to lifestyle modifications such as dietary changes, physical activity and behaviour therapy, overweight individuals with BMIs greater than 27 kg/m^2 but with life threatening diseases, or obese individuals with BMIs greater than 30 kg/m^2 can undergo pharmacotherapy [2].
<box 35% round right |> </box|Figure 12: Orlistat, one of the pharmacological treatments for obesity
from https://www.medexpress.co.uk/javax.faces.resource/treatments/335x335xorlistat-120mg-pills.jpg.xhtml,qln=img.pagespeed.ic.3lJxOPoYEm.jpg>
A meta analysis investigated 21 randomized control trials (RCT) that involved a total of 11 533 participants using either one of the two drugs: orlistat or sibutramine, or a placebo. These RCTs had a follow-up period of at least 1 year in obese and overweight adults.
Olistat functions as a gastrointestinal lipase inhibitor and reduces fat absorption by approximately 30% (Figure 12). Patients can use it for up to two years [43]. On the other hand, sibutramine functions as a serotonin and noradrenaline reuptake inhibitor which induces weight loss through enhanced satiety and increased basal energy expenditure. Sibutramine is approved for clinical use for up to 1 year [44].
Pharmacotherapy trials comparing the effect of combined dietary and pharmacotherapy treatment to dietary treatment alone, showed that patients who received treatment underwent a greater weight loss compared to those who only had a reduced-energy diet. This was when orlistat or sibutramine was combined with a reduced-energy diet. More specifically, the long term weight loss for those receiving combined therapy of dietary and pharmacotherapy was about 6 to 7 kg, compared to about 2 to 3 kg for those who received dietary therapy only [26].
Maintenance of weight loss
Studies that assessed orlistat therapy for at least 2 years and up to 5 years showed that weight loss attained by year 1 was better maintained over the subsequent 3 years in patients who received ongoing drug therapy. Specifically, Davidson et al. showed that patients who had ongoing treatment of orlistat for 2 years were associated with less regain of weight loss (32%) compared with diet only therapy (63%) [45].
In addition, a 2-year study conducted by James et al., showed that 43% of patients who received 6 months of weight loss induction using diet-only therapy, followed by sibutramine-diet therapy had better maintained 80% or more of weight loss, compared to only 16% in the diet-only group who received diet-placebo therapy [46]. This shows that combined therapy is more effective than diet-only group.
Bariatric Surgery
<box 30% round right |>
</box|Figure 12: Orlistat, one of the pharmacological treatments for obesity
from https://www.medexpress.co.uk/javax.faces.resource/treatments/335x335xorlistat-120mg-pills.jpg.xhtml,qln=img.pagespeed.ic.3lJxOPoYEm.jpg>
A meta analysis investigated 21 randomized control trials (RCT) that involved a total of 11 533 participants using either one of the two drugs: orlistat or sibutramine, or a placebo. These RCTs had a follow-up period of at least 1 year in obese and overweight adults.
Olistat functions as a gastrointestinal lipase inhibitor and reduces fat absorption by approximately 30% (Figure 12). Patients can use it for up to two years [43]. On the other hand, sibutramine functions as a serotonin and noradrenaline reuptake inhibitor which induces weight loss through enhanced satiety and increased basal energy expenditure. Sibutramine is approved for clinical use for up to 1 year [44].
Pharmacotherapy trials comparing the effect of combined dietary and pharmacotherapy treatment to dietary treatment alone, showed that patients who received treatment underwent a greater weight loss compared to those who only had a reduced-energy diet. This was when orlistat or sibutramine was combined with a reduced-energy diet. More specifically, the long term weight loss for those receiving combined therapy of dietary and pharmacotherapy was about 6 to 7 kg, compared to about 2 to 3 kg for those who received dietary therapy only [26].
Maintenance of weight loss
Studies that assessed orlistat therapy for at least 2 years and up to 5 years showed that weight loss attained by year 1 was better maintained over the subsequent 3 years in patients who received ongoing drug therapy. Specifically, Davidson et al. showed that patients who had ongoing treatment of orlistat for 2 years were associated with less regain of weight loss (32%) compared with diet only therapy (63%) [45].
In addition, a 2-year study conducted by James et al., showed that 43% of patients who received 6 months of weight loss induction using diet-only therapy, followed by sibutramine-diet therapy had better maintained 80% or more of weight loss, compared to only 16% in the diet-only group who received diet-placebo therapy [46]. This shows that combined therapy is more effective than diet-only group.
Bariatric Surgery
<box 30% round right |> </box|Figure 13: Four highly used surgical procedures used to treating obesity from http://www.cmaj.ca/content/suppl/2007/09/04/176.8.S1.DC1/obesity-lau-onlineNEW.pdf>
Bariatric surgery is a treatment method that is considered for adult patients who have a BMI over 35kg/m^2 with severe comorbid diseases such as life-threatening cardiopulmonary problems, severe sleep apnea, or severe diabetes mellitus, or for those in the severely obese category with a BMI greater than 40 kg/m2. For teenagers, the Canadian Clinical Practice Guidelines on the Management and Prevention of Obesity in Adults and Children recommends that bariatric surgery be limited to an appropriately trained and experienced surgical team. After 6 months of using lifestyle modifications, healthcare practitioners assess the health of the patient and evaluate whether a satisfactory progress of weight loss or goal of 10% of body weight has been reached. In the case that satisfactory progress or goal has not been achieved, physicians will consider the eligibility of patients to undergo bariatric surgery. This is only considered if other nonsurgical weight loss attempts have failed. The goal of bariatric surgery is to relieve a patient suffering from obesity from his or her morbid body weight, improve their comorbidity and improve their quality of life. There are different surgical procedures (Figure 13). It is important to note that this treatment option requires lifelong medical surveillance [26].
A study on obese Swedish patients investigated the conventional, nonsurgical management with surgery for morbid obesity in 2004 found that surgical management is more efficacious than medical management. Patients who received surgical treatment produced greater weight loss, improved lifestyle and dramatic improvement of comorbid disease. At 10 years of follow-up, the surgical cohort showed that they maintained a weight loss greater than 16.1% of their original body weight. In contrast, those who received the conventional, nonsurgical management had a weight gain of 1.6%. This 16.3% weight difference demonstrates the effectiveness and maintenance of surgical procedures [47].
Summary of Treatment Options**
</box|Figure 13: Four highly used surgical procedures used to treating obesity from http://www.cmaj.ca/content/suppl/2007/09/04/176.8.S1.DC1/obesity-lau-onlineNEW.pdf>
Bariatric surgery is a treatment method that is considered for adult patients who have a BMI over 35kg/m^2 with severe comorbid diseases such as life-threatening cardiopulmonary problems, severe sleep apnea, or severe diabetes mellitus, or for those in the severely obese category with a BMI greater than 40 kg/m2. For teenagers, the Canadian Clinical Practice Guidelines on the Management and Prevention of Obesity in Adults and Children recommends that bariatric surgery be limited to an appropriately trained and experienced surgical team. After 6 months of using lifestyle modifications, healthcare practitioners assess the health of the patient and evaluate whether a satisfactory progress of weight loss or goal of 10% of body weight has been reached. In the case that satisfactory progress or goal has not been achieved, physicians will consider the eligibility of patients to undergo bariatric surgery. This is only considered if other nonsurgical weight loss attempts have failed. The goal of bariatric surgery is to relieve a patient suffering from obesity from his or her morbid body weight, improve their comorbidity and improve their quality of life. There are different surgical procedures (Figure 13). It is important to note that this treatment option requires lifelong medical surveillance [26].
A study on obese Swedish patients investigated the conventional, nonsurgical management with surgery for morbid obesity in 2004 found that surgical management is more efficacious than medical management. Patients who received surgical treatment produced greater weight loss, improved lifestyle and dramatic improvement of comorbid disease. At 10 years of follow-up, the surgical cohort showed that they maintained a weight loss greater than 16.1% of their original body weight. In contrast, those who received the conventional, nonsurgical management had a weight gain of 1.6%. This 16.3% weight difference demonstrates the effectiveness and maintenance of surgical procedures [47].
Summary of Treatment Options**
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
As seen in figure 14, there are different approaches to treating obesity. First, it is important to set a weight loss goal to reduce body weight by approximately 10% from baseline during the first six months of treatment. Healthcare practitioners typically recommend their patients to first undergo lifestyle modifications: proper nutrition, physical fitness, and cognitive behaviour therapy. After six months of treatment, healthcare practitioners will assess the patient’s progress and determine whether satisfactory progress or weight loss goal has been reached. In the case that it has been reached, the patient would be closely monitored on a regular basis to make sure that their weight is maintained. In the event that satisfactory progress is not attained, physicians will assess the patient’s eligibility to either undergo pharmacotherapy or bariatric surgery. Physicians typically opt for bariatric treatment in the event that nonsurgical treatments have failed. It is important to note that best weight loss and maintenance results are achieved when pharmacotherapy or bariatric treatment is used in conjunction with lifestyle modifications.

Figure 14: A holistic approach to treating obesity.
References
1. Ng, M., Fleming, T., Robinson, M., Thomson, B., Graetz, N., & Margono, C. et al. (2014). Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: a systematic analysis for the Global Burden of Disease Study 2013.The Lancet, 384(9945), 766-781. http://dx.doi.org/10.1016/s0140-6736(14)60460-8
2. Seidell, J. & Halberstadt, J. (2015). The Global Burden of Obesity and the Challenges of Prevention. Annals Of Nutrition And Metabolism, 66(2), 7-12. http://dx.doi.org/10.1159/000375143
3. WHO: Global Database on Body Mass Index. (2017). Apps.who.int. Retrieved 1 February 2017, from http://apps.who.int/bmi/index.jsp?introPage=intro_3.html
4. Child & Teen BMI | Healthy Weight | CDC. (2017). Centers for Disease Control and Prevention. Retrieved 1 February 2017, from https://www.cdc.gov/healthyweight/assessing/bmi/childrens_bmi/about_childrens_bmi.html
5. Jitnarin, N., Poston, W., Haddock, C., Jahnke, S., & Tuley, B. (2012). Accuracy of body mass index-defined overweight in fire fighters. Occupational Medicine, 63(3), 227-230. http://dx.doi.org/10.1093/occmed/kqs213
6. Spiegelman, B. & Flier, J. (2001). Obesity and the Regulation of Energy Balance. Cell, 104(4), 531-543. http://dx.doi.org/10.1016/s0092-8674(01)00240-9
7. Pietiläinen, K., Kaprio, J., Borg, P., Plasqui, G., Yki-Järvinen, H., & Kujala, U. et al. (2008). Physical Inactivity and Obesity: A Vicious Circle. Obesity, 16(2), 409-414. http://dx.doi.org/10.1038/oby.2007.72
8. Cohen-Cole, E. & Fletcher, J. (2008). Is obesity contagious? Social networks vs environmental factors in the obesity epidemic. Journal Of Health Economics, 27(5), 1382-1387. http://dx.doi.org/10.1016/j.jhealeco.2008.04.005
9. Masuo, K. (2000). A family history of obesity, a family history of hypertension and blood pressure levels. American Journal Of Hypertension, 13(6), S164. http://dx.doi.org/10.1016/s0895-7061(00)01125-0
10. Weaver, J. (2008). Classical Endocrine Diseases Causing Obesity. Obesity And Metabolism, 212-228. http://dx.doi.org/10.1159/000115367
11. Schwartz, T., Nihalani, N., Jindal, S., Virk, S., & Jones, N. (2004). Psychiatric medication-induced obesity: a review. Obesity Reviews, 5(2), 115-121. http://dx.doi.org/10.1111/j.1467-789x.2004.00139.x
12. Dare, S., Mackay, D., & Pell, J. (2015). Relationship between Smoking and Obesity: A Cross-Sectional Study of 499,504 Middle-Aged Adults in the UK General Population. PLOS ONE, 10(4), e0123579. http://dx.doi.org/10.1371/journal.pone.0123579
13. Vermeulen, A. (2005). The epidemic of obesity: Obesity and health of the aging male. The Aging Male, 8(1), 39-41. http://dx.doi.org/10.1080/13685530500049037
14. Schumann, N., Brinsden, H., & Lobstein, T. (2014). A review of national health policies and professional guidelines on maternal obesity and weight gain in pregnancy. Clinical Obesity, n/a-n/a. http://dx.doi.org/10.1111/cob.12062
15. Why Is Sleep Important? - NHLBI, NIH. (2017). National Heart, Lung and Blood Institute. Retrieved 1 February 2017, from https://www.nhlbi.nih.gov/health/health-topics/topics/sdd/why
16. Gurevich-Panigrahi, T., Panigrahi, S., Wiechec, E., & Los, M. (2009). Obesity: pathophysiology and clinical management. Current Medical Chemistry, 16, 506-521. Retrieved from http://liu.diva-portal.org/smash/get/diva2:583167/FULLTEXT01.pdf
17. Odegaard, J., & Chawla, A. (2012). Adipose tissue metabolism in the obese. TheScientist. Retrieved 18 January 2017, from http://www.the-scientist.com/?articles.view/articleNo/33653/title/adipose-tissue-metabolism-in-the-obese/
18. Kahn, B. B., & Flier, J. S. (2000). Obesity and insulin resistance. Journal of Clinical Investigation, 106(4), 473–481.
19. Després, J., & Marette, A. (1999). Obesity and Insulin Resistance. Insulin Resistance, 51-81. doi:10.1007/978-1-59259-716-1_4
20. Klok, M. D., Jakobsdottir, S., & Drent, M. L. (2007). The role of leptin and ghrelin in the regulation of food intake and body weight in humans: a review. Obesity Reviews, 8(1), 21-34. doi:10.1111/j.1467-789x.2006.00270.x
21. Kaszmi, A., Sattar.A., Hashim, R., Khan., S.P.., Younus, M., Khan, F.A. (2013). Serum Leptin values in the healthy obese and non-obese subjects of Rawalpindi. J Pak Med Assoc. 63(2), 245-8
22. Tschop, M., Weyer, C., Tataranni, P. A., Devanarayan, V., Ravussin, E., & Heiman, M. L. (2001). Circulating Ghrelin Levels Are Decreased in Human Obesity. Diabetes, 50(4), 707-709. doi:10.2337/diabetes.50.4.707
23. Walley, A.J., Blakemore, A.I.F. & Froguel, P. (2006). Genetics of obesity and the prediction of risk for health. Human Molecular Genetics. Retrieved 27January, 2017, from https://academic.oup.com/hmg/article/15/suppl_2/R124/626082/Genetics-of-obesity-and-the-prediction-of-risk-for
24. Rankinen, T., Zuberi, A., Chagnon, Y.C., Weisnagel, S.J., Argyropoulos, G., Walts, B., Perusse, L., & Bouchard, C. (2006). The human obesity gene map: the 2005 update. Obesity, 14(4), 529-644.
25. Pi-Sunyer, F. X., Becker, D. M., Bouchard, C., Carleton, R. A., Colditz, G. A., Dietz, W. H., … & Higgins, M. (1998). Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults. American Journal of Clinical Nutrition, 68(4), 899-917.
26. Lau, D. C., Douketis, J. D., Morrison, K. M., Hramiak, I. M., Sharma, A. M., Ur, E., & members of the Obesity Canada Clinical Practice Guidelines Expert Panel. (2007). 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children [summary]. Canadian Medical Association Journal, 176(8), S1-S13.
27. Poirier, P., & Després, J. P. (2001). Exercise in weight management of obesity. Cardiology clinics,19(3),459-470.
28. Hey, H., Petersen, H. D., Andersen, T., & Quaade, F. (1987). Formula diet plus free additional food choice up to 1000 kcal (4.2 MJ) compared with an is energetic conventional diet in the treatment of obesity. A randomised clinical trial. Clinical Nutrition,6(3),195-199.
29. Lau, D. C., Douketis, J. D., Morrison, K. M., Hramiak, I. M., Sharma, A. M., Ur, E., & members of the Obesity Canada Clinical Practice Guidelines Expert Panel. (2007). 2006 Canadian clinical practice guidelines on the management and prevention of obesity in adults and children [summary]. Canadian Medical Association Journal, 176(8), S1-S13.
30. Toubro, S., & Astrup, A. (1997). Randomised comparison of diets for maintaining obese subjects' weight after major weight loss: ad lib, low fat, high carbohydrate diet fixed energy intake. Bmj,314(707329.
31. 9 Popular Weight Loss Diets Reviewed by Science. (2016, October 04). Retrieved January 27, 2017, from https://authoritynutrition.com/9-weight-loss-diets-reviewed/
32. Poirier, P., & Després, J. P. (2001). Exercise in weight management of obesity. Cardiology clinics, 19(3), 459-470.
33. Tremblay, A., Nadeau, A., Despres, J. P., St-Jean, L., Theriault, G., & Bouchard, C. (1990). Long-term exercise training with constant energy intake. 2: Effect on glucose metabolism and resting energy expenditure. International journal of obesity, 14(1), 75-84.
34. Gwinup, G. (1987). Weight loss without dietary restriction: efficacy of different forms of aerobic exercise. The American journal of sports medicine, 15(3), 275-279.
35. Pate, R. R., Pratt, M., Blair, S. N., Haskell, W. L., Macera, C. A., Bouchard, C., … & Kriska, A. (1995). Physical activity and public health: a recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine. Jama, 273(5), 402-407.
36. Nozaki, T., Sawamoto, R., & Sudo, N. (2013). Cognitive behavioral therapy for obesity. Nihon rinsho. Japanese journal of clinical medicine, 71(2), 329-334.
37. Cooper, Z., Fairburn, C. G., & Hawker, D. M. (2003). Cognitive-behavioral treatment of obesity: A clinician's guide. Guilford Press.
38. Diabetes Prevention Program (DPP) Research Group. (2002). The diabetes prevention program (DPP). Diabetes care, 25(12), 2165-2171.
39. Look AHEAD Research Group. (2003). Look AHEAD (Action for Health in Diabetes): design and methods for a clinical trial of weight loss for the prevention of cardiovascular disease in type 2 diabetes. Controlled clinical trials,24(5), 610-628.
40. Renjilian, D. A., Perri, M. G., Nezu, A. M., McKelvey, W. F., Shermer, R. L., & Anton, S. D. (2001). Individual versus group therapy for obesity: effects of matching participants to their treatment preferences. Journal of consulting and clinical psychology, 69(4), 717.
41. Wrotniak, B. H., Epstein, L. H., Paluch, R. A., & Roemmich, J. N. (2004). Parent weight change as a predictor of child weight change in family-based behavioral obesity treatment. Archives of pediatrics & adolescent medicine, 158(4), 342-347.
42. Epstein, L. H., Roemmich, J. N., Stein, R. I., Paluch, R. A., & Kilanowski, C. K. (2005). The challenge of identifying behavioral alternatives to food: clinic and field studies. Annals of Behavioral Medicine, 30(3),201-209
43. Guerciolini, R. (1997). Mode of action of orlistat. International journal of obesity and related metabolic disorders: journal of the International Association for the Study of Obesity, 21, S12-23.
44. Finer, N. (2002). Sibutramine: its mode of action and efficacy. International Journal of Obesity, 26(S4), S29.
45. Davidson, M. H., Hauptman, J., DiGirolamo, M., Foreyt, J. P., Halsted, C. H., Heber, D., … & Heymsfield, S. B. (1999). Weight control and risk factor reduction in obese subjects treated for 2 years with orlistat: a randomized controlled trial. Jama, 281(3), 235-242.
46. James, W. P. T., Astrup, A., Finer, N., Hilsted, J., Kopelman, P., Rössner, S., … & STORM Study Group. (2000). Effect of sibutramine on weight maintenance after weight loss: a randomised trial. The Lancet, 356(9248), 2119-2125
47. Sjöström, L., Lindroos, A. K., Peltonen, M., Torgerson, J., Bouchard, C., Carlsson, B., … & Sullivan, M. (2004). Lifestyle, diabetes, and cardiovascular risk factors 10 years after bariatric surgery. New England Journal of Medicine, 351(26), 2683-2693.