Table of Contents
Transmission and Pathogenesis of SARS-CoV-2
(Created by Kyle Cordeiro, Karol Derech, Cailyn Eley, Shahithra Kirubalingam & Abigail Oladesu)
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is the virus responsible for the zoonotic respiratory disease that is now commonly known as Coronavirus disease 2019 shortened to Covid-19. Since the outbreak in December 2019 originating from Wuhan, China the virus has spread to 219 countries with almost 100 million cases that have been reported and over 2 million recorded deaths (Huang et al., 2020).
SARS-CoV-2 is the third coronavirus outbreak in the last 20 years. The SARS-CoV-2 virus is similar to the pathogenic SARS-CoV of 2003 and Middle Eastern Respiratory Syndrome coronavirus (MERS-CoV) of 2012 (Hulswit, 2016). SARS-CoV-2 is less lethal than both SARS-CoV or MERS-CoV but is significantly more transmissible than both diseases.
SARS-CoV-2 is a positive-sense single-stranded RNA virus. It is part of the Betacoronavirus genus which is characterized by the enveloped positive-strand RNA viruses that affect mammals. It is 29,881 bp in length and encodes 9860 amino acids. Its morphology consists of both nonstructural and structural proteins (Gavor et al., 2020). The non-structural proteins include proteases, RNA-dependent RNA polymerase, helicases as well as other enzymes (Chan et al., 2020). However, it is the structural proteins that are most relevant to transmission and pathogenesis.
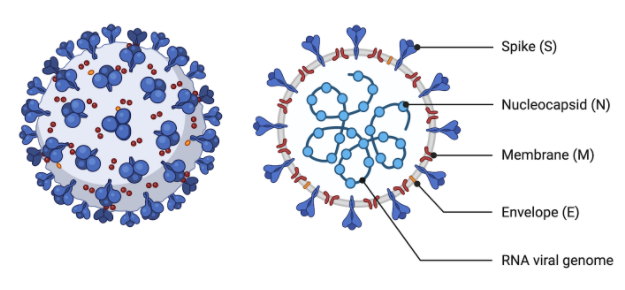
Figure 1: Structure of SARS-CoV-2 Virus. Made on Biorender.com (2020).
Structural Proteins
- Spike (S): Envelope glycoprotein involved in attachment, fusion, and entry into the host cell. Originally a precursor protein, it is cleaved into an S1 and S2 subunit that facilitates attachment and membrane fusion respectively (Harrison et al., 2020).
- Nucleocapsid (N): Forms stable complexes with genomic RNA and increases virion assembly efficiency
- Envelope (E): Involved in assembly, budding, and envelope formation
- Membrane (M): Structural membrane layer of the virion particle
Spike Protein
The spike protein is of particular importance in the COVID-19 infection cycle, yet also one of the most elusive elements of SARS-CoV-2. While it is known that SARS-CoV-2 only targets angiotensin-converting enzyme 2 (ACE2) for viral attachment and entry, the SARS-CoV-2 spike protein itself is less understood. Depending on the stage of the viral life cycle the spike protein can exist in different conformations to enable various functions of the spike protein (Huang et al., 2020). Of these conformations, most research has centered around the prefusion and postfusion spike conformations in order to better understand how the virus enters host cells. In the prefusion conformation, three S1/S2 spike dimers form a trimer spike that erects from the viral envelope (Huang et al., 2020). The S1 subunit contains a receptor-binding domain (RBD) while the S2 subunit is composed of a hydrophobic fusion peptide and two heptad repeat regions that facilitate membrane fusion and viral entry when brought close to the host cell membrane as a result of conformational changes (Harrison et al., 2020).
Angiotensin-Converting Enzyme 2
ACE2 is a type I membrane glycoprotein composed of 805 amino acids and belonging to the angiotensin-converting enzyme family of dipeptidyl carboxypeptidases. This family of enzymes is closely tied to the renin-angiotensin system (RAS) that plays an important role in the regulation of blood pressure. Through the RAS, angiotensin-converting enzyme 1 produces the strong vasoconstrictor angiotensin II from its precursor molecule angiotensin I, directly increasing blood pressure through vasoconstriction (Ni et al., 2020). The natural role of ACE2 is to use its extracellular domain to convert angiotensin II into the vasodilator angiotensin(1-7) by removing 1 amino acid (Ni et al., 2020). This has the effect of returning blood pressure to homeostasis by introducing a vasodilator to compensate for vasoconstriction. However, the prefusion spike trimer also shares a high affinity for the ACE2 receptor and can make use of the amino acid cleavage to cleave the spike protein into S1 and S2 subunits, causing vast conformational change into the postfusion state and resulting in membrane fusion and eventual viral entry into the host cell (Huang et al., 2020).
Being the sole target of betacoronavirus spike protein attachment, ACE2 expression is absolutely essential for infection to manifest (Ni et al., 2020). For this reason, the tissue tropism of SARS-CoV-2 aligns closely with the level of ACE2 expression in tissues. ACE2 can be found in cells all over the body, although it is most prominently found in lung epithelial alveolar cells, enterocytes, arterial and venous endothelial cells, and arterial cells (Hamming et al., 2004). There is evidence of viral RNA in each of these tissues, although the primary tropism of SARS-CoV-2 is in the lungs and respiratory tract (Harrison et al., 2020). Some structural variations of human ACE2 have been identified that have a lower binding affinity with spike protein suggesting the virus has an easier time infecting some than others (Hussain et al., 2020), and the receptor is currently being researched as a potential treatment possibility.
Life Cycle of SARS-CoV-2
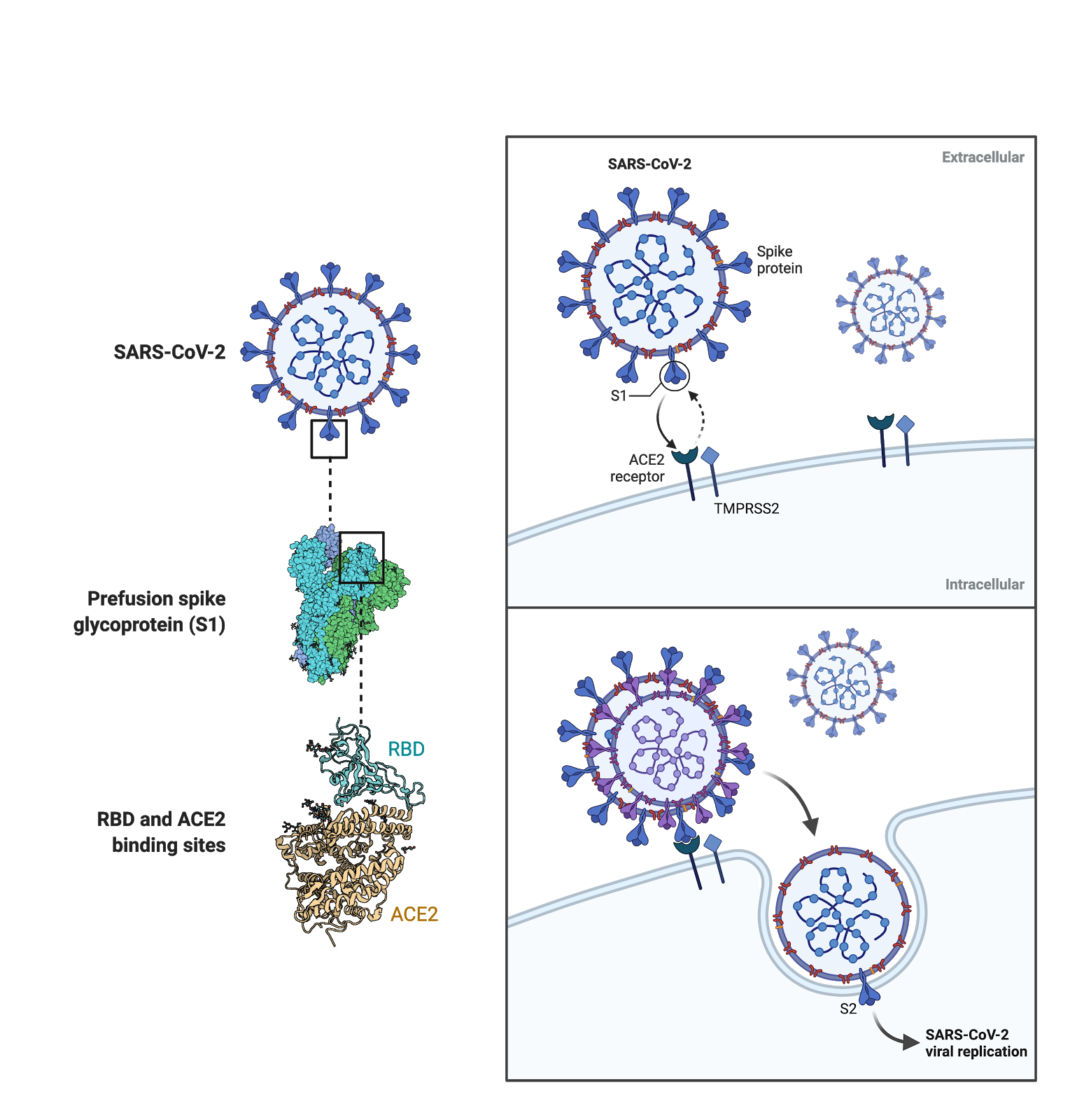
Figure 2: Process of spike attachment, membrane fusion, and viral entry into host cell. Made on BioRender.com (2020).
The life cycle of SARS-CoV-2 can be recognized at five different stages:
- Viral Attachment and Entry
- Genome Release
- Translation of Viral Proteins and Genome Replication
- Assembly of New Virions
- Release of Progeny
Viral Attachment and Entry
The first step of viral entry is binding of the receptor-binding domain of the N-Terminal S1 spike subunit to a pocket of the ACE2 receptor. Upon direct contact with ACE2, cleavage of viral S1/S2 site by the surface transmembrane protease serine 2 (TMPRSS2) initiates conformational change in the spike protein that allow membrane fusion between host cell and S2 subunit.
Genome Release
Once the viral particle has entered the cytoplasm of the host cell, the viral envelope dissolves, releasing the positive-sense RNA viral genome into the cytosol (Harrison et al., 2020). The viral genome is then translated by host cell ribosomes, creating viral proteins. Of these viral proteins, ORF1a and ORF1b on the viral genome translate into virus specific replicase proteins (Harrison et al., 2020). These polyproteins, pp1a and pp1b, are cleaved by a virus-encoded protease into individual replicase complex nonstructural proteins (nsps), which expedites the translation of viral genome into viral protein (Harrison et al., 2020). Essentially the viral genome acts as a template for RNA replication and encodes the RNA-dependent RNA polymerase (RdRP) necessary for genomic replication.
Translation of Viral Proteins and Genome Replication
Replication begins in the virus-induced double-membrane vesicles (DMVs), derived from the endoplasmic reticulum (ER) (Harrison et al., 2020). The initial positive-strand genome acts as a template for the production of full-length negative-strand RNA and subgenomic RNA (Harrison et al., 2020).
Assembly of New Virions
Subgenomic RNA is translated into structural and accessory proteins, which is inserted into the ER-Golgi intermediate compartment (ERGIC), where virion assembly occurs (Harrison et al., 2020). Following virion assembly from structural and accessory proteins, a positive-sense RNA genome is added into the newly synthesized virions (Harrison et al., 2020).
Release of Progeny
Progeny viral cells are now complete, and will be released from the initially infected host cell into extracellular space, finding new suitable cells to attach to, where the process begins again.
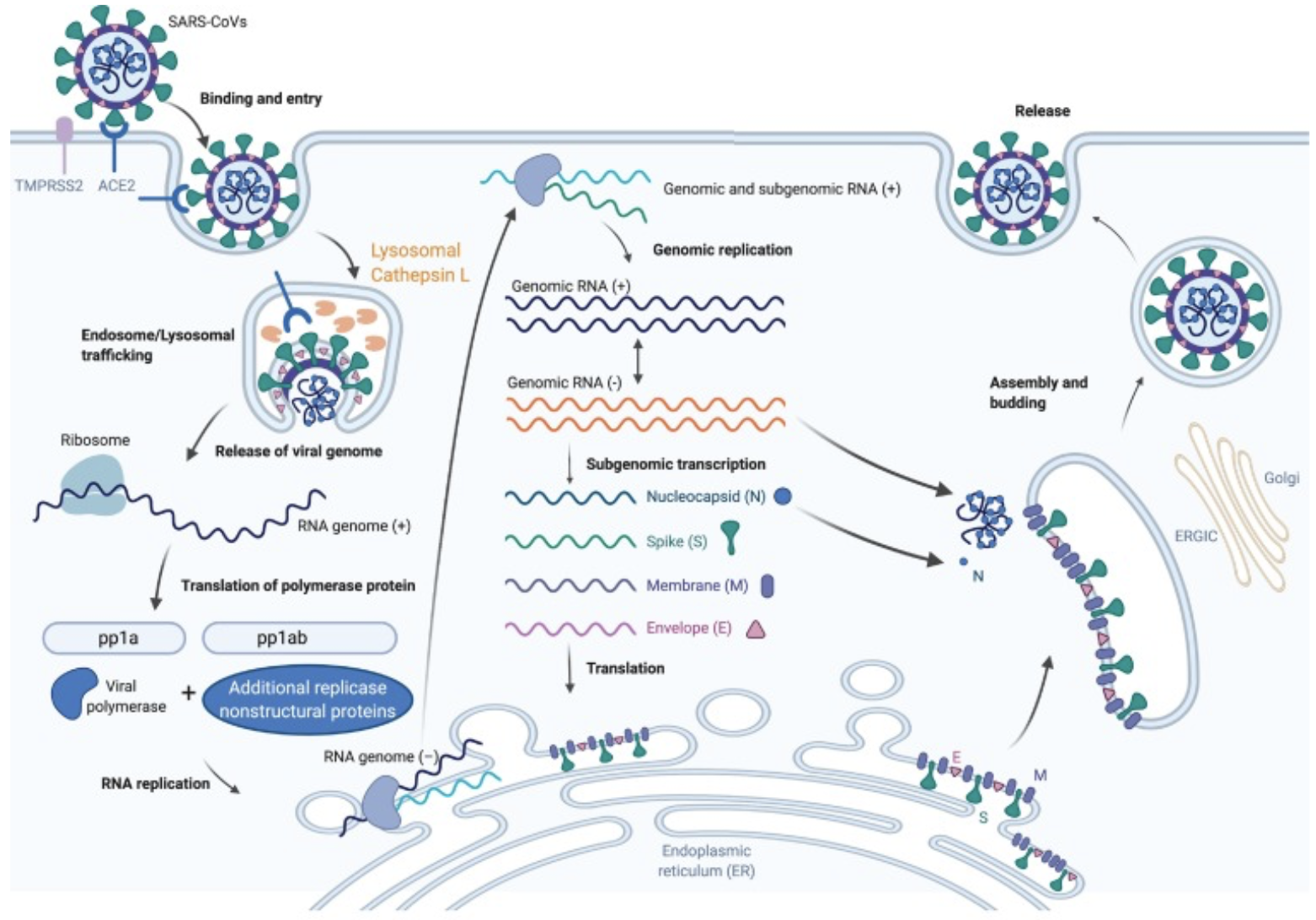
Figure 3: Graphic overview of the life cycle of SARS-CoV-2 (Harrison et al., 2020).
Transmission of SARS-CoV-2
The transmission dynamics of SARS-CoV-2 vary greatly under different circumstances. An issue in measuring the transmission of a pathogen is that transmissibility is not a biological constant and is influenced by the three factors of the epidemiological triad - agent, host, and environmental factors (Mishra, Haleem, & Javaid, 2020). The transmission of COVID-19, therefore, depends on specific properties of the virus itself (agent factors), physiology and behavior of the host (host factors), and the environment that they are interacting in. These factors directly influence how quickly the virus spreads, represented in the doubling time and reproductive numbers of the virus. While the doubling time is typically observed as about 4.5-5 days in populations following recommended safety precautions, the doubling time has been shown to decrease to as low as 2 days in populations that are not (Mishra, Haleem & Javaid, 2020).
SARS-CoV-2 was initially thought to be zoonotic in nature (transmissible mainly from animals to humans), but as the pandemic progressed, the human-to-human transmission was found to be the main source of spread currently (F. Zhou et al., 2020). After contracting the virus, there is an incubation period that typically lasts five days (can take a maximum of two weeks) before the host is able to transmit the virus to others (WHO, 2020). Interestingly, human-to-human transmission can occur whether the host is symptomatic (actively displaying symptoms), pre-symptomatic (passed incubation period of the virus but not yet showing symptoms), or asymptomatic (does not show symptoms of the virus throughout the period of infection) (WHO, 2020).
Ideally, infected individuals begin to show symptoms after the incubation period and are able to assess their health status in order to self-isolate for the course of the disease. However, pre-symptomatic and asymptomatic cases pose a high risk of transmission as the host may be completely unaware of their infection and unknowingly spread it to those around them. There is also evidence showing that viral load in the upper respiratory tract is highest a week into the infection, around the time of symptom onset or shortly after, suggesting this could be a period of heightened infectivity (Cevik et al., 2021). This period of heightened viral load coincides with the periods symptoms may begin to show increasing the risk of secondary infection. On the other hand, asymptomatic individuals can go a substantial period of time with no knowledge of the infection, providing possibilities for spread. However, it remains incredibly difficult to measure the exact rate of transmissibility in pre-symptomatic and asymptomatic cases as the transmission occurs before the source of infection is known. Despite this, evidence shows that although asymptomatic individuals do not transmit the virus with the same efficiency as symptomatic individuals, the reproductive number for asymptomatic individuals is greater than 1, meaning that they will likely infect at least one new person and propagate the disease forward (Levy et al., 2020).
Modes of Transmission
SARS-CoV-2 can be transmissible either horizontally, where the virus is transmitted among individuals of the same generation, or vertically, where transmission occurs from mothers to their offspring (Rahman et al., 2020).

Figure 4: SARS-CoV-2 Transmission Routes. (2020). Adapted from https://www.cell.com/trends/immunology/fulltext/S1471-4906(20)30233-7
Horizontal Transmission
Droplet Transmission
Amongst these routes, the primary route of transmission is through direct contact from virus-containing respiratory droplets that are greater than 5-10 um from the oral cavity and respiratory tract (WHO, n.d.). It is possible to contract the disease if they were in close contact with pre-symptomatic individuals in the incubation period, asymptomatic individuals, or those who have symptoms of COVID-19. Droplet transmission can occur when the virus-containing droplets are inhaled, ingested, or land onto the conjunctiva or mucous membranes of a non-infected individual who is in close contact with an infected individual (Luo et al., 2020). Respiratory droplets can be propelled from 2 m up to 8 m horizontally (Bahl et al., 2020), showing the importance of social distancing when trying to prevent spread.
An indirect mode of transmission by the respiratory droplets is through fomites, which are objects that carry the infection. Due to the larger size of the respiratory droplets, they are subject to gravitational pull and fall onto nearby surfaces and floors. The virus is able to remain stable and viable for about 48-72 hours on stainless steel and plastic surfaces, with a half-life of approximately 1.1-1.2 hours (Van Doremalen et al., 2020). Transmission occurs when an individual touches these virus-contaminated surfaces and objects, then subsequently touch their mouth, nose, or eyes (Guo et al., 2020). Self-inoculation of the disease through fomites could result from poor hand hygiene or by failing to follow adequate disease-controlling practices following exposure to fomites (Guo et al., 2020). This is proposed as a likely mode of transmission, but there is still little evidence of direct fomites transmission as individuals who come into contact with fomites are usually in close contact with infected individuals (WHO, n.d.).
Aerosols
Airborne transmission is another proposed route transmission in which smaller virus-containing droplets, less than 5 um in size known as aerosols, are the source of infection (WHO, n.d.). Aerosols can be released through air coughs, and sneezes from both symptomatic and asymptomatic individuals to contaminate the environment (Belser et al., 2020). Due to their smaller size, aerosols are able to diffuse into the surrounding air and persist at high concentrations for about three hours. They are also found on surfaces and objects contributing to fomites transmission (Van Doremalen et al., 2020). The half-life of the virus is almost the same in aerosols as it is in fomites, with estimates being approximately 1.1-1.2 hours (Van Doremalen et al., 2020). Hospital procedures on the respiratory pathway, dental care, or hemodialysis can produce virus-containing aerosols, and contribute to nosocomial transmission by infected individuals who are not adequately protected (Wang et al., 2020). There are various environmental factors that could affect the viability of the airborne virus including temperature, humidity, radiation, and open-air ventilation (Marthi, 1994). The virus is able to either gain or infectivity due to these environmental factors, and the environmental tolerance of the virus depends on its phenotype, composition, and overall characteristics of the surrounding area (Shuit et al., 2020). These environmental factors could play an important role in the understanding of COVID-19 transmission and are something to be further explored. Overall, airborne transmission of COVID-19 is still an area of research as some sources have shown that the virus has not been detected during air sampling for distances greater than 2 m (F. Zhou et al., 2020).
Anal Secretions
The fecal-oral route has also been proposed as a mode of transmission after viral RNA has been detected in anal secretions of infected patients as well as a high ACE2 expression in gastrointestinal cells (Xiao et al., 2020). Although this route of transmission is still continuing to be explored, some researchers have found that viral shedding from the digestive tract may be higher than in the respiratory tract and that the virus can persist in the digestive tract for much longer (Wu et al., 2020). Transmission through this route has been proposed to occur through pathways such as fomites, fingers (direct contact), fields (environment), and fluids (Guo et al., 2020).
Vertical Transmission
Vertical transmission occurs when the virus is passed from mother to fetus. However, this is an uncommon occurrence and could be due to specific conditions. Some studies have suggested that there is a high expression of ACE2 receptors in the human maternal-fetal interphase, proving as evidence for this being a potential mode of transmission (Levy et al., 2020). There are also possibilities for transmission through direct contact and respiratory droplets (Poon et al., 2020). There is currently no evidence for breastfeeding transmission from mother to child due to the lack of viral DNA found in breast milk in PCR studies (Poon et al., 2020).
Pathogenesis
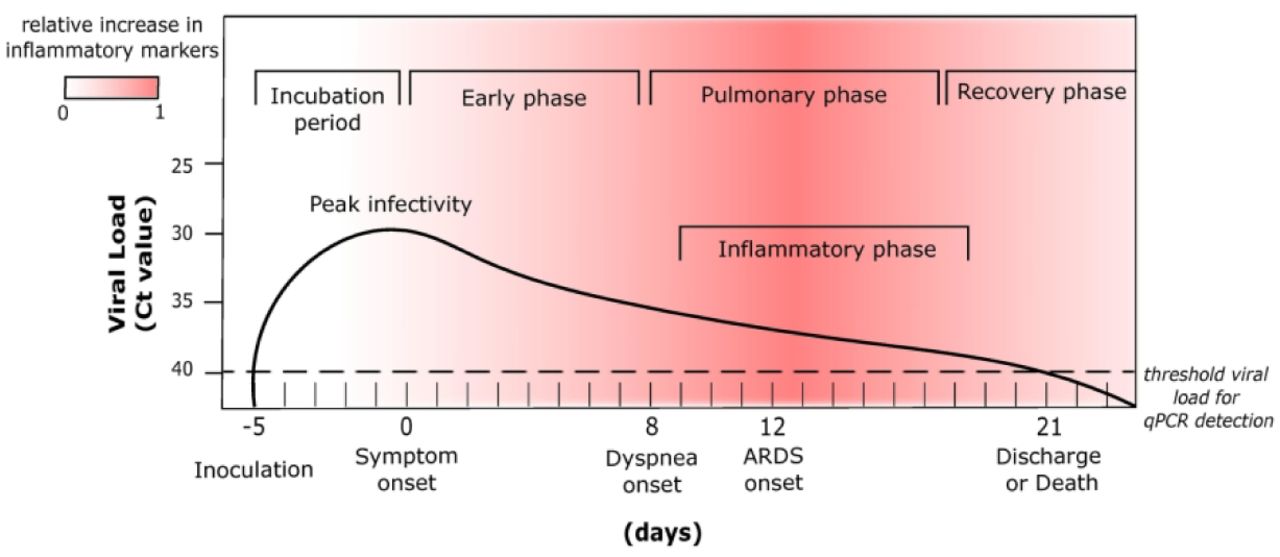
Figure 5: Average timeline of SARS-CoV-2 pathogenesis, including viral load over time and clinical manifestations of infection (Acosta & Singer, 2020).
The exact mechanism of SARS-CoV-2 pathogenesis is yet to be determined, but hypothetical mechanisms have been proposed based on the literature surrounding COVID-19 infection. SARS-CoV-2 enters the cells via the receptor ACE2 and will replicate in tissues that possess a sufficient level of this receptor. Therefore, it is speculated that the distribution of ACE2 is related to symptoms of viral infection (Guan et al., 2020). Initially, the virus may replicate in the mucosa of the upper respiratory tract where it may then pass through the lower respiratory tract and gain access to the lungs (Guan et al., 2020). Viral replication and release within the lungs are associated with the symptoms such as fever, cough, and muscle pain reported in COVID-19 patients 5-6 days after exposure (Cevik, Bamford, & Ho, 2020). These symptoms are typically associated with moderate disease. At this point, an infected individual may be able to completely clear the virus and make a full recovery within another 4-5 days.
Individuals who are unable to clear the virus may see a progression in the disease at around 7-14 days after exposure (Guan et al., 2020). It has been proposed that the virus may gain access to the bloodstream (primary viremia) after replicating in the lungs, where it can then spread to other tissues expressing ACE2 (Monteil et al., 2020). Evidence of viral replication has been found in the intestines, kidneys, and hearts of COVID-19 patients, which may explain gastrointestinal and cardiovascular complications reported in some individuals (Monteil et al., 2020). Some complications may include kidney injury and proteinuria, as well as nausea and anorexia (Richardson et al., 2020). During this phase of the disease, pulmonary complications are common. Infected individuals may develop pulmonary infiltrates and experience shortness of breath and severe hypoxemia at around 8 days post-exposure (F. Zhou et al., 2020).
The highest morbidity and mortality rates are experienced shortly after and are attributed to a dysregulated immune response. Dangerous levels of inflammation could lead to life-threatening conditions like cardiac and renal failure and/ or Acute Respiratory Distress Syndrome (ARDS) (Yang et al., 2020). ARDS has been reported as the most common fatal sequelae associated with COVID-19 and has resulted in the majority of Intensive Care Unit (ICU) admissions (Rodriguez-Morales et al., 2020).
Individuals who experience severe disease may subsequently enter into a recovery phase or succumb to complications associated with COVID-19. Recovery is characterized by decreased viral load, decreased inflammation, and increased tissue repair.
Immunopathogenesis
Research has shown that SARS-CoV-2 can aggravate the host immune system and cause a dysfunctional immune response in infected individuals. This dysregulated immune response appears to be a factor in COVID-19 pathogenesis and clinical manifestation, particularly in cases of severe disease.
Many COVID-19 patients develop lymphopenia as a result of the disease. Lymphocytes such as T cells are a primary viral defense mechanism and COVID-19 patients demonstrate a significant depletion of these cells. Additionally, many T cells that are still present in COVID-19 patients become overactivated and eventually display an exhausted phenotype, thus failing to perform their function (Diao et al., 2020). One study found that the number of T cells in the blood of patients post-infection with SARS-CoV-2 was inversely correlated with the level of inflammatory cytokines, suggesting that the prolonged inflammatory response may contribute to the depletion of lymphocytes (Y. Zhou et al., 2020).
SARS-CoV-2 infection also promotes drastically elevated cytokine levels that can lead to a phenomenon known as a cytokine storm. In response to the viral challenge, cytokines are produced as a natural immune response. In some cases of SARS-CoV-2 infection, this can lead to the rapid conversion of naive CD4+ T cells into Th1 cells, resulting in a positive feedback loop, where the Th1 cells stimulate monocytes to secrete more inflammatory cytokines which leads to the activation of more Th1 cells (Y. Zhou et al., 2020). The abundance of cytokines produced can promote tissue damage and inflammation, which can lead to multiple organ failure in patients whose immune systems cannot gain control over the overactive antiviral response. As a result, a cytokine storm may contribute to the systemic tissue damage observed in some COVID-19 patients post-mortem.
In addition, severe COVID-19 has also been characterized by a less robust interferon (IFN) response. In a typical antiviral immune response, IFNs induce intracellular Janus Kinase-Signal Transducers and Activators of Transcription (JAK-STAT) pathways that stimulate the transcription of Interferon Stimulated Genes (ISGs) (De Wit, Van Doremalen, Falzarano, & Munster, 2016). This is meant to control viral replication and assist in viral clearance, however, SARS-CoV-2 exhibits IFN antagonism and has been shown to blunt this response in some patients (Miorin et al., 2020). One study found that a viral protein called Orf6 is able to prevent STAT1 nuclear translocation to some degree and therefore impair IFN signaling (Miorin et al., 2020).
Pathology
Symptomology
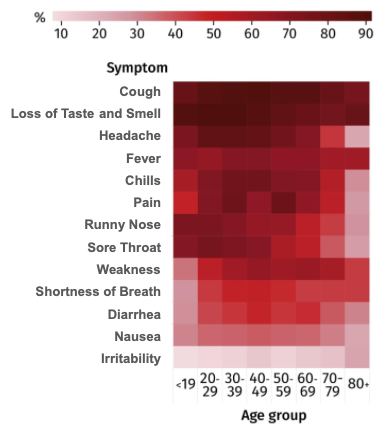
Figure 6: COVID-19 Symptoms Frequency For Various Age Groups (CBC, 2020).
Following infection of SARS-CoV-2, the first symptoms of COVID-19 will appear after 5-7 days, when the viral load within an individual is at its peak (Garcia, 2020). These initial symptoms are defined as “flu-like”, consistent of fever, cough, chills, mild body aches, and chills (Garcia, 2020). Due to the abundance of ACE2 receptors in human oral and nasal cells, the sudden and complete loss of taste and smell is a symptom associated with many cases of COVID-19 (Garcia, 2020). This loss of taste and smell is typically one of the first symptoms noticed, especially among younger and healthier individuals, whose natural immune response will only allow mild “flu-like” symptoms to persist during viral infection.
In more moderate to severe cases of COVID-19, viral cells have become prevalent in the blood, and are able to reach other areas of the body with cells of high ACE2 expression outside of the Respiratory tract (Wu et al., 2020). In these cases, SARS-CoV-2 will begin to replicate in the kidneys, GI tract, and heart. Possible symptoms include severe shortness of breath, hypoxemia, as well as other cardiovascular or gastrointestinal complications, such as diarrhea, anorexia, and nausea (Wu et al., 2020).
In the most severe cases of COVID-19, viral cells have perpetrated multiple major organs, and a variety of complications resulting from this can result in patient death. As well, a dysregulated immune response can result in a “cytokine storm”, which has severe and commonly fatal complications (Wu et al., 2020). Other fatal causes of death due to COVID-19 include kidney and/or heart failure, cardiac arrest, acute respiratory distress syndrome (ARDS), or severe pneumonia (Wu et al., 2020).
Acute Respiratory Distress Syndrome
Acute Respiratory Distress Syndrome (ARDS) is a common complication in patients with severe COVID-19. ARDS usually develops within an individual due to another disease or major injury and causes low blood oxygen (Mattay et al., 2019. In lungs with ARDS, there is increased permeability to liquid and protein across the lung endothelium, which causes fluid buildup in the lung interstitium. This fluid buildup then translocates to the alveolar epithelium, along with the buildup of other proteins, neutrophils, and red blood cells are the main physical characteristics of ARDS (Mattay et al., 2019). Due to these complications in the alveolar epithelium, patients will experience arterial hypoxemia, impaired excretion of carbon dioxide, and a number of additional complications that lead to an increase in pulmonary dead space (Mattay et al., 2019). Impaired secretion of carbon dioxide, as well as rising levels of pulmonary dead space, are key predictors in the mortality of patients with ARDS (Mattay et al., 2019).
In severe COVID-19 patients, ARDS arises when pneumonia symptoms worsen and are usually prevalent around 14 days following infection. Shortness of breath due to pneumonia from COVID-19 is an indicator that ARDS may result in the patient (Mattay et al., 2019). If a patient with COVID-19 does develop ARDS, they are often unable to breathe on their own, and will likely require a ventilator to support the circulation of oxygen into their blood. ARDS in severe COVID-19 patients can often be fatal, but even in patients who survive, they may have lasting pulmonary scarring, and ongoing respiratory issues and concerns.
Risk Factors & Outcomes
Factors Influencing Variation in Pathology
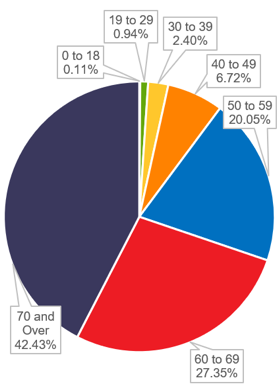
Figure 8: COVID-19 Death Toll Sorted by Age Groupings (AJMC, 2020).
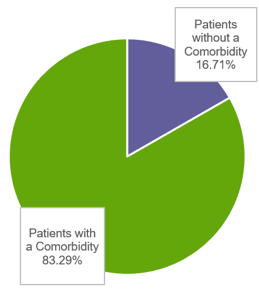
Figure 7: COVID-19 Death Toll Sorted by Presence of Comorbidity (AJMC, 2020).
Pathology of COVID-19 varies greatly amongst every individual, however, there are key trends and factors that would place particular individuals at higher risk of developing severe and potentially fatal COVID-19 infections. Although a majority of COVID-19 cases only result in mild to moderate symptoms, it is still of benefit to identify risk factors, allowing individuals who possess one or more of these risk factors to take greater precautions in decreasing the likelihood they contract SARS-CoV-2.
The age of an individual is a major statistical determinant of how COVID-19 will resolve within a patient. Among a sample of COVID-19 diagnoses, 42.11% of cases involved patients aged 39 years of age and lower. These patients resulted in only 3.45% of COVID-19 deaths among this sample (Gelburd, 2020). Inversely, individuals aged 70 years of age or older shared 4.82% of COVID diagnoses within this sample, yet accounted for 42.43% of the deaths (Gelburd, 2020). Although the age of an individual should not be used exclusively to determine the risk of fatal outcome due to COVID-19, it should be noted that individuals of older age may possess other risk factors at much higher tendencies, and additional emphasis should be placed on protecting them. This correlation is likely due to the fact that the natural human immune system generally weakens as individuals age (Gelburd, 2020).
The presence of comorbidity is also a large statistical determinant of whether an individual will succumb to COVID-19. Within a sample of COVID-19 deaths, 83.29% of these deaths were of patients who presented comorbidity at death (Gelburd, 2020). Individuals possessing immunodeficiency due to an existing chronic illness should be considered at higher risk of severe, or fatal COVID-19 infection, and precautions must be in place to protect these individuals. However, it is imperative that they remain with access to the proper medical intervention to treat their existing illness or complication, or their state may worse, or result fatally.
Cytokine Profile
Different cytokine profiles have been associated with the development of moderate versus severe COVID-19. Shortly after infection with SARS-CoV-2, the majority of people will exhibit a significant increase in pro-inflammatory cytokines. At first, people who will go on to develop the moderate disease and people who will go on to develop the severe disease will see an increase in certain key cytokines. Some common cytokines observed in response to the virus are Tumor Necrosis Factor-α (TNF-α) and Interleukin-6 (IL-6) (Giamarellos-Bourboulis et al., 2020). The cytokine profiles of people with moderate and severe diseases begin to differ at around day 10 after symptom onset. The moderate disease is characterized by a sharp decline in pro-inflammatory markers whereas these same markers remain elevated in people with severe COVID-19 (Lucas et al., 2020).
Early differences in cytokine expression may be a predictor of clinical outcome for COVID-19 patients. Patients who experienced moderate disease progression tend to have lower expression of pro-inflammatory cytokines early in infection and higher expression of tissue repair genes (Lucas et al., 2020). Thus, these patients are more likely to recover from the disease. Patients who develop severe disease tend to have higher pro-inflammatory cytokine expression early on in infection and do not experience the same enrichment in repair genes (Lucas et al., 2020). This could explain why some patients are unable to recover.
Challenges and Implications
Transmission
Although extensive research has been conducted to identify the various modes and severity of transmission routes for the COVID-19 virus, it is important to continue looking for and confirming important routes of transmission. Transmission routes can help identify and control the spread of the virus through preparedness, readiness, and response actions (WHO, 2020). By identifying routes of transmission as well as transmission rates, researchers will be able to gather pertinent information on human motility, epidemiological and genetic data at various levels of the population.
Going forward, this data on the transmission of the virus can be used to implement strategies and public health guidelines to prevent spread and control infections. Having knowledge on how respiratory droplets or aerosols are transmitted can help design adequate PPE (personal protective equipment) for front line workers as well as for the general public. This can also outline the requirements for social distancing rules, as well as capacity rules for stores and other public areas.
Findings from fomite and the fecal-oral transmission routes can be used to implement enhanced sanitation in public areas, such as stores, washrooms, and schools. It can also help develop accurate and relevant public health messaging when it comes to how and why COVID-19 spreads, and how individuals can protect themselves. In extreme cases, information on the transmission of the virus can also help government officials make decisions on a local or regional level to implement self-isolation protocols or city-wide lockdowns.
Pathogenesis
Understanding the full model of pathogenesis in regard to SARS-CoV-2 continues to be a top priority for medical research institutions worldwide. Gaining the complete knowledge on the functions of the virus, common tendencies of this viral infection, as well as risk factors individuals may possess, would provide us with an outstanding ability to ensure each patient who contracts COVID-19 has not only the highest likelihood of survival but also the ability to control any potential long-term damage the virus may cause.
As extensive research on the full pathogenetic model of the virus continues, it is imperative that proper animal models are found and used, to better understand these functions, and allow results to be confidently translated into understanding the human model. By doing so, and findings can be translated to the discovery of more effective therapeutics, accurate clinical diagnosis, and proper clinical intervention and treatment of the disease (Wu et al., 2020).
The discovery of effective therapeutics has been a global continued effort since the inception of the COVID-19 pandemic. With lacking knowledge in the complete understanding of SARS-CoV-2, the therapeutic potential was initially focused on how the virus differs from SARS-CoV and MERS-CoV and using previously developed therapeutics to use where similarities lied among SARS-CoV-2 with its predecessors. Remdesivir and Ribavirin were used, in part to similarities among SARS-CoV-2’s replicase proteins with SARS-CoV. However, the binding domain of SARS-CoV-2 showed to be distinct from that of previous coronaviruses, and inhibition of cellular attachment and entry proved to be a challenge (Wu et al., 2020). Future research should be focused on therapeutics targeting this binding domain, and preventing initial cellular entry.
Alternatively, therapeutics inhibiting viral entry by modifying ACE2 in host cells is a viable idea to lower SARS-CoV-2 infections. Conflicting data have been found in regard to this treatment, in addition to concerns of chloroquine toxicity with therapeutics that were previously developed and used (Wu et al., 2020). As global research in identifying potential therapeutics for SARS-CoV-2, as well as other coronaviruses, continues, drug candidates with efficacy in inhibiting viral bonding by modification or inhibition of ACE2 would prove to be extremely beneficial.
Presentation Slides
References
Acosta, M. A. T., & Singer, B. D. (2020). Pathogenesis of COVID-19-induced ARDS: implications for an aging population. European Respiratory Journal. https://doi.org/DOI: 10.1183/13993003.02049-2020
Bahl, P., Doolan, C., de Silva, C., Chughtai, A. A., Bourouiba, L., MacIntyre, C. R. (2020). Airborne or droplet precautions for health workers treating COVID-19?. Journal of Infectious Disease. https://doi.org/10.1093/infdis/jiaa189.
Belser, J. A., Rota, P. A., Tumpey, T. M. (2013). Ocular tropism of respiratory viruses. Microbiology Molecular Biology Review, 77(1), 144-156.
Cevik, M., Tate, M., Lloyd, O., Maraolo, A. E., Schafers, J., Ho, A. (2021). SARS-CoV-2, SARS-CoV, and MERS-CoV viral load dynamics, duration of viral shedding and infectiousness: a systematic review and meta-analysis. The Lancet Microbe 2(1), E13-E22. https://doi.org/10.1016/S2666-5247(20)30172-5
Cevik, M., Bamford, C. G. G., & Ho, A. (2020). COVID-19 pandemic—a focused review for clinicians. Clinical Microbiology and Infection, 26(7), 842–847. https://doi.org/10.1016/j.cmi.2020.04.023
De Wit, E., Van Doremalen, N., Falzarano, D., & Munster, V. J. (2016). SARS and MERS: Recent insights into emerging coronaviruses. Nature Reviews Microbiology, 14(8), 523–534. https://doi.org/10.1038/nrmicro.2016.81
Diao, B., Wang, C., Tan, Y., Chen, X., Liu, Y., Ning, L., Chen, Y. (2020). Reduction and Functional Exhaustion of T Cells in Patients With Coronavirus Disease 2019 (COVID-19). Frontiers in Immunology. https://doi.org/10.3389/fimmu.2020.00827
Garcia, L.F. (2020). Immune Response, Inflammation, and the Clinical Spectrum of COVID-19. Frontiers in Immunology, 11, 1441. https://doi.org/10.3389/fimmu.2020.01441
Gavor, E., Choong, Y., Er, S., Sivaraman, H. & Sivaraman, J., 2020. Structural Basis of SARS-CoV-2 and SARS-CoV Antibody Interactions. Trends in Immunology, 41(11), 1006-1022.
Gelburd, J. R. D. (2020a). Contributor: Links Between COVID-19 Comorbidities, Mortality Detailed in FAIR Health Study. AJMC. https://www.ajmc.com/view/contributor-links-between-covid-19-comorbidities-mortality-detailed-in-fair-health-study
Giamarellos-Bourboulis, E. J., Netea, M. G., Rovina, N., Koulouris, N., Gogos, C., Koutsoukou, A. (2020). Complex immune dysregulation in COVID-19 patients with severe respiratory failure. Cell Host and Microbe, 27, 992-1000.
Guan, W., Ni, Z., Hu, Y., Liang, W., Ou, C., He, J., Zhong, N. (2020). Clinical Characteristics of Coronavirus Disease 2019 in China. New England Journal of Medicine. https://doi.org/10.1056/nejmoa2002032
Guo, Z.-D., Wang, Z.-Y., Zhang, S.-F., Li, X., Li, L., Li, C., Cui, Y., Fu, R.-B., Dong, Y.-Z., Chi, X.-Y. (2020). Aerosol and surface distribution of severe acute respiratory syndrome coronavirus 2 in hospital wards, Wuhan, China, 2020. Emerging Infectious Diseases, 26(7).
Hamming, I., Timens, W., Bulthuis, M. L., Lely, A. T., Navis, G., & van Goor, H. (2004). Tissue distribution of ACE2 protein, the functional receptor for SARS coronavirus. A first step in understanding SARS pathogenesis. The Journal of pathology, 203(2), 631–637. https://doi.org/10.1002/path.1570
Harrison, A. G., Lin, T., & Wang, P. (2020). Mechanisms of SARS-CoV-2 Transmission and Pathogenesis. Trends in Immunology, 41(12), 1100–1115. https://doi.org/10.1016/j.it.2020.10.004
Huang, C., Wang, Y., Li, X., Ren, L., Zhao, J., Hu, Y., et al. (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 395, 497–506. doi: 10.1016/S0140-6736(20)30183-5
Huang, Y., Yang, C., Xu, X., Xu, W. & Liu, S. (2020). Structural and functional properties of SARS-CoV-2 spike protein: potential antivirus drug development for COVID-19. Acta Pharmacologica Sinica, 41, 1141-1149. https://doi.org/10.1038/s41401-020-0485-4
Hulswit, R., Haan, C. D. & Bosch, B. (2016). Coronavirus Spike Protein and Tropism Changes. Retrieved from https://www.sciencedirect.com/science/article/pii/S0065352716300434
Hussain, M., Jabeen, N., Raza, F., Shabbir, S., Baig, A. A., Amanullah, A., Aziz, B. (2020). Structural variations in human ACE2 may influence its binding with SARS-CoV-2 spike protein. Journal of Medicine and Virology.. https://doi.org/10.1002/jmv.25832
Levy, A., Yagil, Y., Bursztyn, M., Barkalifa, R., Scharf, S., & Yagil, C. (2020). ACE2 expression and activity are enhanced during pregnancy. American Journal of Physiology, 295(6). Luo L, Liu D, Liao X, Wu X, Jing Q, Zheng J, et al. (2020). Modes of contact and risk of transmission in COVID-19 among close contacts (pre-print). MedRxiv. https://doi.org/10.1101/2020.03.24.20042606.
Lucas, C., Wong, P., Klein, J., Castro, T. B. R., Silva, J., Sundaram, M., Iwasaki, A. (2020). Longitudinal analyses reveal immunological misfiring in severe COVID-19. Nature, 584, 463–469. https://doi.org/10.1038/s41586-020-2588-y
Marthi B. (1994). Resuscitation of microbial bioaerosols. In: Lighthart B., Mohr A.J., editors. Atmospheric Microbial Aerosols. Springer; Boston, MA: 1994. pp. 192–225.
Matthay MA, Zemans RL, Zimmerman GA, Arabi YM, Beitler JR, Mercat A, Herridge M, Randolph AG, Calfee CS. (2019). Acute respiratory distress syndrome. Nature Review Disease Primers,18. doi: 10.1038/s41572-019-0069-0.
Miorin, L., Kehrer, T., Sanchez-Aparicio, M. T., Zhang, K., Cohen, P., Patel, R. S., García-Sastre, A. (2020). SARS-CoV-2 Orf6 hijacks Nup98 to block STAT nuclear import and antagonize interferon signaling. Proceedings of the National Academy of Sciences of the United States of America, 117(45), 28344–28354. https://doi.org/10.1073/pnas.2016650117
Mishra, D., Haleem, A., & Javaid, M. (2020). Analysing the behaviour of doubling rates in 8 major countries affected by COVID-19 virus. Journal of Oral Biology and Craniofacial Research, 10(44), 478-483. https://doi.org/10.1016/j.jobcr.2020.08.007
Monteil, V., Kwon, H., Prado, P., Hagelkrüys, A., Wimmer, R. A., Stahl, M., Penninger, J. M. (2020). Inhibition of SARS-CoV-2 Infections in Engineered Human Tissues Using Clinical-Grade Soluble Human ACE2. Cell, 181(4), 905–913. https://doi.org/10.1016/j.cell.2020.04.004
Ni, W., Yang, X., Yang, D., Bao, J., Li, R., Xiao, Y., Hou, C., Wang, H., Liu, J., Yang, D., Xu, Y., Cao, Z. & Gao, Z. (2020). Role of angiotensin-converting enzyme 2 (ACE2) in COVID-19. Critical Care, 24(422). https://doi.org/10.1186/s13054-020-03120-0
Poon, L. C., Yang, H., Kapur, A., Melamed, N., Dao, B., Divakar, H. et al. (2020). Global interim guidance on coronavirus disease 2019 (COVID-19) during pregnancy and puerperium from FIGO and allied partners: information for healthcare professionals. International Journal of Gynecology and Obstetrics, 149(3), 273-286.
Rahman, H. S., Aziz, M. S., Hussein, R. H., Othman, H. H., Omer, S. H. S., Khalid, E. S., Abdulrahman, N. A., Amin, K. & Abdullah, R. (2020). The transmission modes and sources of COVID-19: A systematic review. International Journal of Surgery Open, 26. https://doi.org/10.1016/j.ijso.2020.08.017
Richardson, S., Hirsch, J. S., Narasimhan, M., Crawford, J. M., McGinn, T., Davidson, K. W., Zanos, T. P. (2020). Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. Journal of the American Medical Association, 323(20), 2052–2059. https://doi.org/10.1001/jama.2020.6775
Rodriguez-Morales, A. J., Cardona-Ospina, J. A., Gutiérrez-Ocampo, E., Villamizar-Peña, R., Holguin-Rivera, Y., Escalera-Antezana, J. P., Sah, R. (2020). Clinical, laboratory and imaging features of COVID-19: A systematic review and meta-analysis. Travel Medicine and Infectious Disease, 34, 101623. https://doi.org/10.1016/j.tmaid.2020.101623
Schuit M., Gardner S., Wood S., Bower K., Williams G., Freeburger D., Dabisch P. (2020). The influence of simulated sunlight on the inactivation of influenza virus in aerosols. Journal of Infectious Disease;221:372–378. doi: 10.1093/infdis/jiz582
Seglins, D., Wesley, A., & Rocha, R. (2020). We looked at every confirmed COVID-19 case in Canada. Here’s what we found. CBC News. https://www.cbc.ca/news/canada/public-health-agency-of-canada-covid-19-statistics-1.5733069
Van Doremalen, N., Bushmaker, T., Morris, D. H., Holbrook, M. G., Gamble, A., Williamson, B. N. et al. (2020). Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. New England Journal of Medicine, 382(16):1564-7. Available from: https://doi.org/10.1056/NEJMc2004973
Wang, W., Xu, Y., Gao, R., Lu, R., Han, K., Wu, G. et al. (2020). Detection of SARS-CoV-2 in different types of clinical specimens. JAMA, 323(18):1843-4. Available from: https://doi.org/10.1001/jama.2020.3786
World Health Organization. (n.d.). Infection Prevention and Control of Epidemic-and Pandemic-prone Acute Respiratory Infections in Health Care. Retrieved February 01, 2021, from https://apps.who.int/iris/bitstream/handle/10665/112656/9789241507134_eng.pdf;jsessionid=41AA684FB64571CE8D8A453C4F2B2096?sequence=1)
World Health Organization. (2020). Transmission of SARS-CoV-2: Implications for infection prevention precautions. Retrieved February 01, 2021, from https://www.who.int/news-room/commentaries/detail/transmission-of-sars-cov-2-implications-for-infection-prevention-precaution
Wu, L., O'Kane, A. M., Peng, H., Bi, Y., Motriuk-Smith, D., & Ren, J. (2020). SARS-CoV-2 and cardiovascular complications: From molecular mechanisms to pharmaceutical management. Biochemical pharmacology, 178, 114114. https://doi.org/10.1016/j.bcp.2020.114114
Xiao, F., Tang, M., Zheng, X., Liu, Y., Li, X., Shan, H. (2020). Evidence for gastrointestinal infection of SARS-CoV-2. Gastroenterology, 158:1831–1833.
Xiao, F., Sun, J., Xu, Y., Li, F., Huang, X., Li, H., Zhao, J., Huang, J., Zhao, J. (2020). Infectious SARS-CoV-2 in Feces of Patient with Severe COVID-19. Emerging Infectious Disease, (8):1920-1922. doi: 10.3201/eid2608.200681. Epub 2020 May 18. PMID: 32421494; PMCID: PMC7392466.
Yang, X., Yu, Y., Xu, J., Shu, H., Xia, J., Liu, H., Shang, Y. (2020). Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. The Lancet Respiratory Medicine, 8(5), 475–481. https://doi.org/10.1016/S2213-2600(20)30079-5
Zhou, F., Yu, T., Du, R., Fan, G., Liu, Y., Liu, Z., Cao, B. (2020). Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. The Lancet, 395(10229), 1054–1062. https://doi.org/10.1016/S0140-6736(20)30566-3
Zhou, J., Otter, J. A., Price, J. R., Cimpeanu, C., Garcia, D. M., Kinross, J., Boshier, P. R., Mason, S., Bolt, F., Holmes, A. H., Barclay, W. S. (2020). Investigating SARS-CoV-2 surface and air contamination in an acute healthcare setting during the peak of the COVID-19 pandemic in London. Clinical Infectious Diseases, ciaa905. https://doi.org/10.1093/cid/ciaa905
Zhou, Y., Fu, B., Zheng, X., Wang, D., Zhao, C., qi, Y., Wei, H. (2020). Aberrant pathogenic GM-CSF + T cells and inflammatory CD14 + CD16 + monocytes in severe pulmonary syndrome patients of a new coronavirus. National Science Review. https://doi.org/10.1101/2020.02.12.945576