Table of Contents
SARS-CoV-2: Pathogenesis & Transmission
History of SARS-CoV-2
COVID-19 (otherwise known as Coronavirus disease 2019) is a contagious disease primarily affecting the respiratory system that is caused by SARS-CoV-2 (severe acute respiratory syndrome coronavirus 2). In December 2019, the first human cases of the COVID-19 pandemic were identified in Wuhan, China. On January 30 2020, the World Health Organization declared COVID-19 as a Public Health Emergency of International Concern, and on March 11, 2020, it was declared as a pandemic (World Health Organization, n.d.). The virus spread worldwide, and in November 2020 the United States was the first country to have at least 10 million confirmed cases, and in December 2020 India was the second country to have at least 10 million confirmed cases (CNN, January 2022). There were many other countries that followed with 10 million confirmed cases (CNN, January 2022), including Brazil (February 2021), the United Kingdom (November 2021), Russia (December 2021), France (January 2022), Turkey (January 2022), and Italy (January 2022).
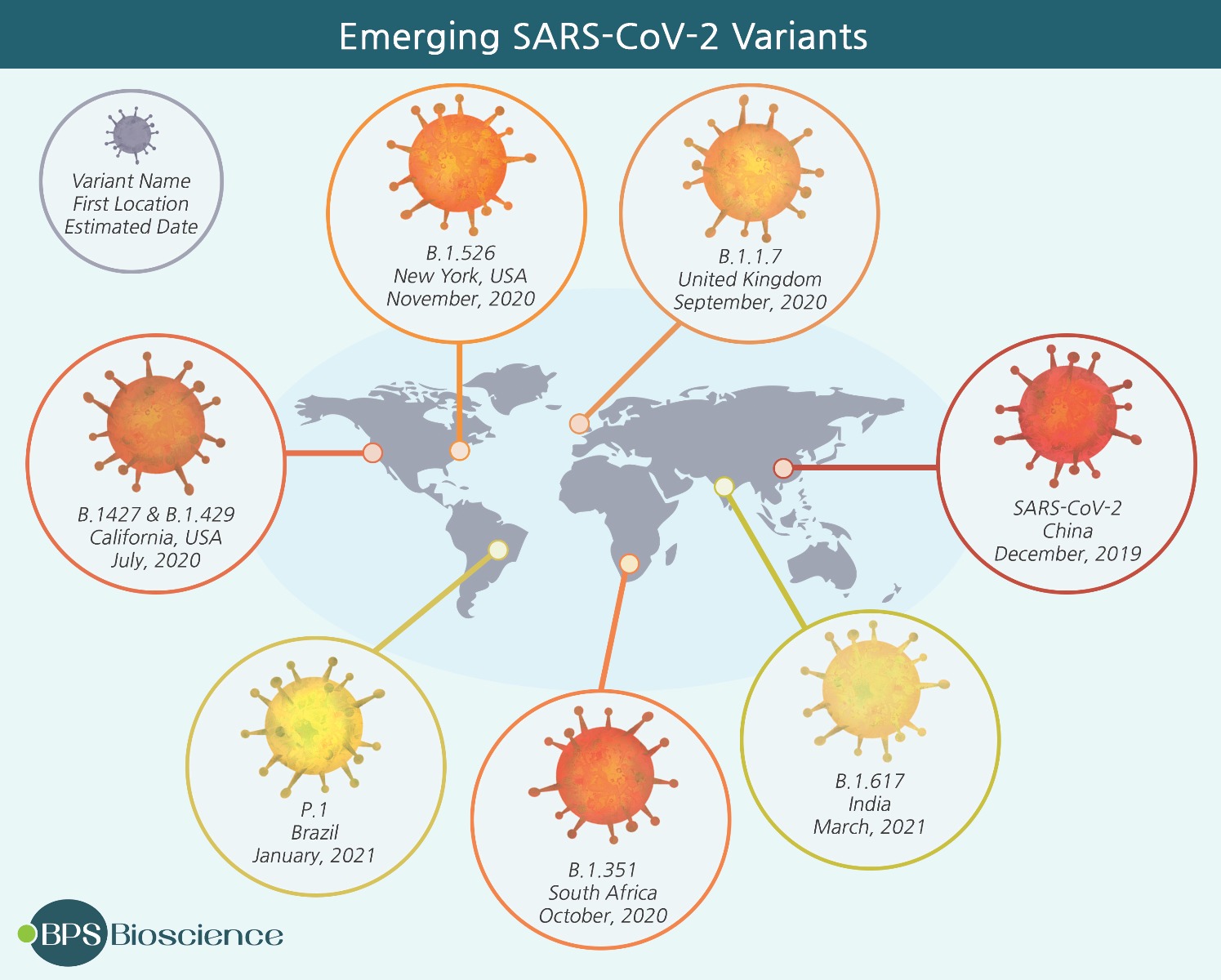
Figure 1. SARS-CoV-2 Variants. Since the emergence of SARS-CoV-2 in 2019, several mutant strains have been discovered in countries around the world (BPS, n.d.))
During this time, there were also a number of developments in vaccination measures to protect individuals from COVID-19 (AJMC, n.d.), however, there was also considerable research on the clinical trial method for these vaccines as well as the possibility and severity of adverse reactions. In Canada, the approved SARS-CoV-2 vaccines include the Moderna Spikevax vaccine, the Pfizer-BioNTech Comiranty vaccine, the AstraZeneca Vaxzevria vaccine, and the Janssen (Johnson & Johnson) vaccine (Health Canada, 2022). The development of the SARS-CoV-2 vaccines also included considerable advances in mRNA vaccines (enabling the muscle cell to create a modified, harmless fragment of the spike protein in order to prepare an immune response), and led to further research on the differences between this vaccination method compared to viral-vector vaccines (containing a modified, harmless version of the spike protein that enters the muscle cell and allows the body to prepare an immune response).
Over the course of the pandemic, there have also been a number of variants of concern (World Health Organization, n.d.), namely the Alpha variant (first recorded in United Kingdom, September 2020), the Beta variant (first recorded in South Africa, May 2020), the Gamma variant (first recorded in Brazil, November 2020), the Delta variant (first recorded in India, October 2020), and the Omicron variant (multiple countries, November 2021). Some variants experienced noticeable spread to various other countries, including the Delta and Omicron variants in particular.
While there are hundreds of coronaviruses circulating among animals, some of those viruses can spread to humans, otherwise known as a spillover event. Namely, the SARS coronavirus (SARS-CoV) was first identified in China, in February 2003 (World Health Organization, n.d.), resulting in severe acute respiratory syndrome (SARS), while the Middle East respiratory syndrome (MERS) was reported in September 2012 (CDC, n.d.) and was caused by the MERS coronavirus (MERS-CoV). The SARS coronavirus generally led to fever, headache, malaise, and muscle pain, as well as some mild respiratory symptoms. The MERS coronavirus generally led to fever, cough, shortness of breath, some gastrointestinal symptoms, and commonly pneumonia. There have also been severe illnesses as a result of this virus which requires mechanical ventilation and support in an intensive care unit (WHO, n.d.).
This article aims to introduce the Genome and Structure, the Viral Life Cycle, Pathogenesis, Clinical Presentation and Risk Factors, and Transmission of SARS-CoV-2.
Genome & Structure
The genome of SARS-CoV-2 shares approximately 80% sequence similarity with SARS-CoV-1 and 50% with MERS-CoV. The genome of SARS-CoV-2 consists of 14 open-reading frames (ORFs), of which 9 encode non-structural proteins forming the replicase complex (Zhang et al., 2020). The remaining ORFs encode four structural proteins and nine accessory proteins. The structural proteins consist of the spike (S), envelope (E), membrane (M), and nucleocapsid (N) (Huang et al., 2020).
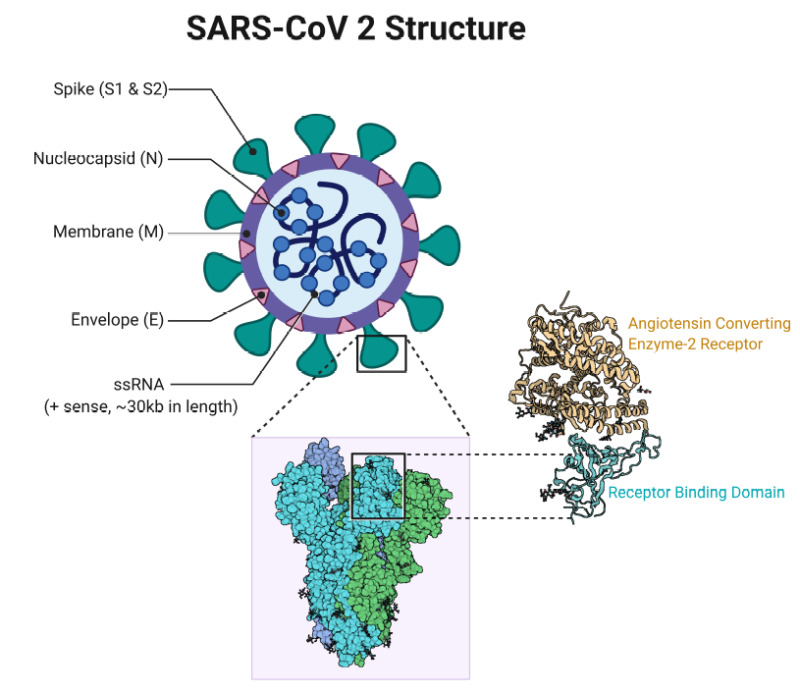
Figure 2. SARS-CoV-2 Structure. Key structural proteins include Spike (S), Nucleocapsid (N), Envelope (E) and Membrane (M). Receptor Binding Domain on Spike binds Angtiotension Converting Enzyme-2 Receptor (Cascella et al., 2022))
The Spike protein consists of S1 and S2 subunits, the former of which binds a cognate receptor on the host cell surface. Cleavage at the S1/S2 site allows for a conformational change in Spike that is a prerequisite for membrane fusion and entry of the viral particle into the cytosol (Lu et al., 2020) (Jackson et al., 2021). The Nucleocapsid complexes with the viral genomic RNA and allows for efficient packaging of the viral genome. The Envelope provides protection to the viral genome prior to infection. The Membrane provides structural stability to the viral particle housing the genome as it travels in search of target cells (Harrison et al., 2020) (Hoffman et al., 2020).
Viral Life Cycle
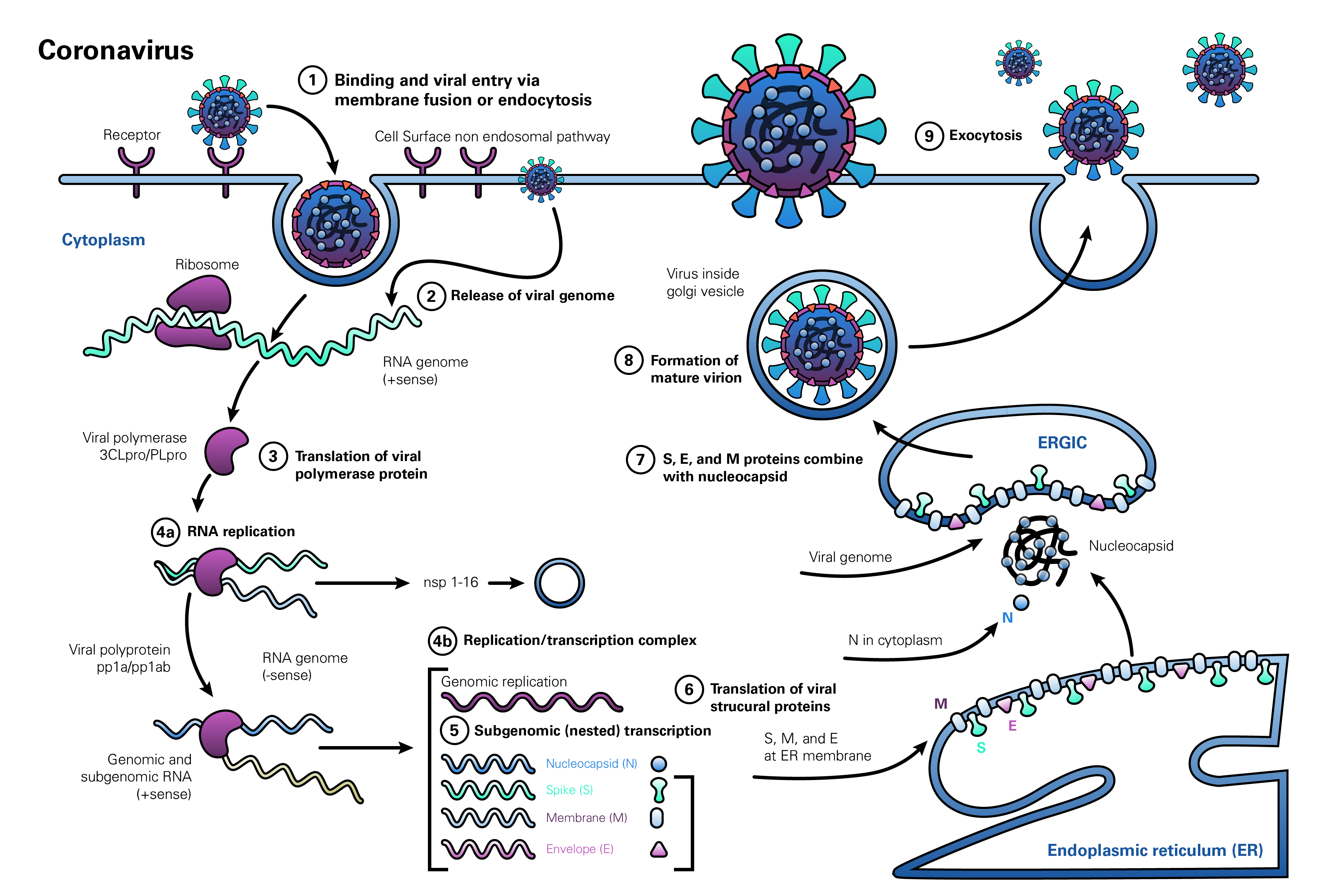
Figure 3. SARS-CoV-2 viral lifecycle. The viral lifecycle begins with binding and attachment on host cell surfaces, followed by cellular uptake and release of viral RNA genome. Production of viral replicases precedes translation of subgenome and RNA genome replication. Translated subgenome forms the assembled virion, which is packed with the replicated RNA genome. The completed viral particle leaves the cell in search of new targets (V'kovski et al., 2020)
Binding and Entry
The Spike protein mediates viral entry into the host cell, by binding the N terminal S1 subunit of the Spike protein to the host cell receptor angiotensin-converting enzyme 2 (ACE2) (Hoffman et al., 2020). Release of the viral genome into the cytosol is dependent on cleavage of S1/S2 subunits, allowing for fusion between the S2 subunit and the plasma membrane followed by entry of the viral envelope into the host cell (Hoffman et al., 2020) (Huang et al., 2020).
Genome Release
Cleavage on the S1/S2 site can occur via one of two mechanisms, relying on either transmembrane protease S2 or cathepsin L. TMPRSS2 enables entry at the plasma cell membrane via S1/S2 cleavage followed by membrane fusion (Shulla et al., 2011). However, if TMPRSS2 is unavailable, cathepsin L found in endolysosomes activates the Spike protein and facilitates S1/S2 cleavage (Huang et al., 2020). Through either mechanism, the viral envelope is released into the cytosol. Upon entering the cytosol, the envelope dissolves and the viral genome is released into the host cell (Harrison et al., 2020).
ORF1a and ORF1b are translated into polyproteins pp1a and pp1b, which are then cleaved to form individual replicase complex non-structural proteins constituting the RNA-dependent RNA polymerases needed for replication of the viral genome (Harrison et al., 2020).
Genome Replication and Subgenomic Transcription
Replication occurs in double-membrane vesicles (DMVs) formed from the host cell’s endoplasmic reticulum (ER). The positive-strand RNA genome that entered the cell serves as template for full-length negative strand RNA production and subgenomic RNA (sgRNA) transcription. sgRNA is translated to produce virion components such as accessory and structural proteins (Wu et al., 2010). The full-length negative strand RNA produced by viral replicases is used as a template to form positive sense RNA genomes (Harrison et al., 2020).
Virion Assembly
The accessory and structural proteins formed at the DMV from sgRNA are assembled in the ER-Golgi intermediate compartment (ERGIC) for assembly of virions. Positive sense RNA genomes are also trafficked to the ERGIC for packaging into newly assembled virions (Harrison et al., 2020).
Release of Viral Particles
Assembled virions are then transported out of the cell via the plasma membrane and into the extracellular matrix to find another susceptible host cell to begin the viral life cycle anew (Harrison et al., 2020).
Pathogenesis
Early Stages of Infection
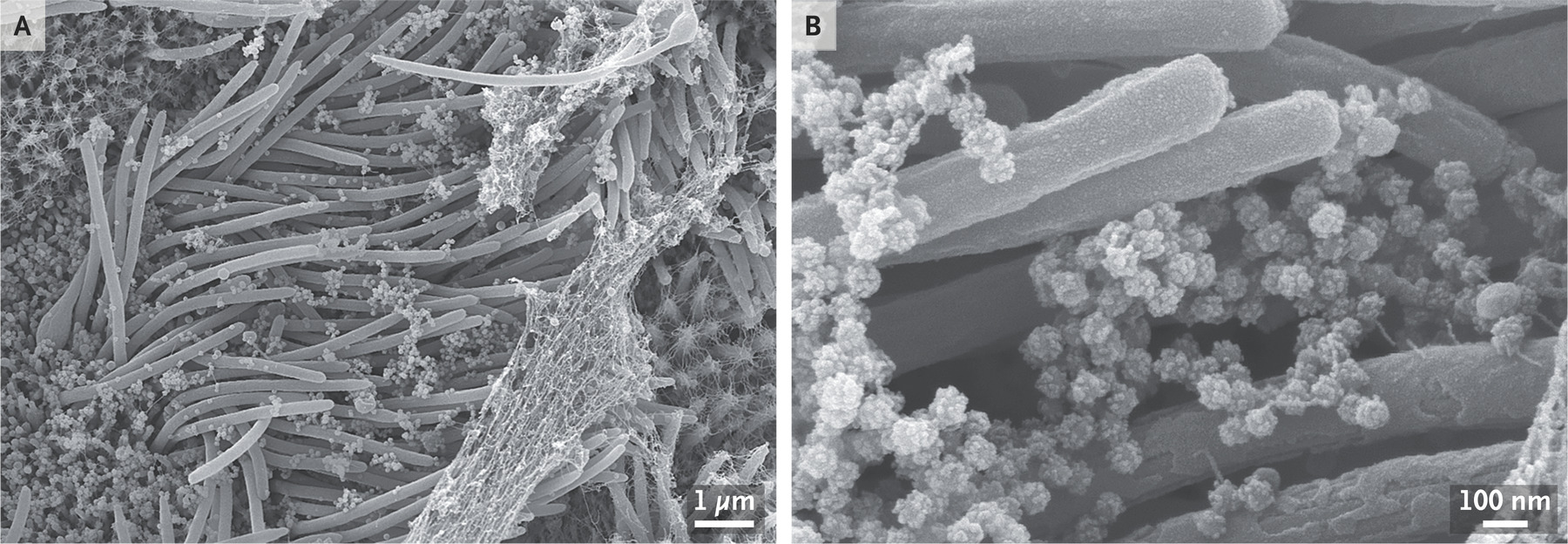
Figure 4. Human Bronchial Epithelial Cells Infected with SARS-CoV-2. Infection of cells was carried out with a multiplicity of infection (ratio of viral particles to epithelial cells) of 3:1. Images generated with scanning electron microscopy. Image A shows infected airway cells and mucus-covered cilia. Image B showcases virion particles generated by infected cells (Ehre, 2020)
Viral tropism and pathogenesis are contingent on access to susceptible cell surfaces. The SARS epidemic mirrors the current COVID-19 pandemic in causing patients to present with respiratory symptoms progressing to severe pneumonia. As such, it is postulated that the primary tropism, or target tissue, of SARS-CoV-2 are the lungs. SARS-CoV-2, much like its predecessor, binds the entry receptor ACE2 (Hoffman et al., 2020). However, unlike SARS-CoV-1, SARS-CoV-2 bears several key mutations in the receptor binding domain (RBD) of its Spike protein, which promotes higher binding affinity, tighter adherence to host cell surfaces, and increased infectivity (Harrison et al., 2020). Like SARS-CoV-1, SARS-CoV-2, upon entering the host organism via the upper respiratory tract, progresses to begin early infection and viral replication in airway and alveolar epithelial cells, alveolar macrophages and vascular endothelial cells. These cell types are prime targets for tropism and “ground zero” for infection due to their expression of the ACE2 entry receptor protein (Hoffman et al., 2020). The very first cells infected may be epithelial cells in the upper respiratory tract, after which infection spreads to the lower respiratory tract, and finally, the lungs. This pathway of SARS-CoV-2 tropism is commonly associated with moderate presentation of the disease.
Dependence of Infection on Innate Cell Characteristics
Interestingly, despite ACE2 mRNA being detected in lung biopsies of human and non-human mammalian hosts, ACE2 is expressed in greater quantities in extra-pulmonary tissue. This suggests that other cell-specific factors, in addition to ACE2 presentation, determine SARS-CoV-2 binding affinity and cellular tropism. In the case of SARS-CoV-1, Shulla et al. (2011) demonstrated that cellular susceptibility to SARS-CoVs may be maintained in spite of very low ACE2 expression, provided that the protease TMPRSS2 is present on the would-be host cell for cleavage at the S1/S2 cleavage site. Additionally, human lung biopsies reveal a subset of type II alveolar cells with increased expression of ACE2. This same population of type II alveolar cells displays increased mRNA expression of genes associated with higher SARS-CoV-2 susceptibility, such as endosomal sorting complex required for transport (ESCRT) machinery genes. Examples include CHMP3, CHMP5, and CHMP1A. This implies that SARS-CoV-2 preferentially infects a small subset of human type II alveolar cells with high distribution of ACE2 for viral replication (Zhao et al., 2020). Yet other alternative cell characteristics may help determine susceptibility to viral infection. For instance, expression of ACE2 is upregulated in airway epithelial cells in response to type I and II interferons (IFNs) released by the immune response to SAR-CoV infection. Finally, another factor extending SARS-CoV-2 tropism is the insertion of RRAR at the S1/S2 cleavage site (Qin et al., 2020) (Hoffman et al., 2020). With this insertion, this site can be cleaved by the furin protease enzyme instead of requiring specific proteases on the target cell, such as TMPRSS2 (Hoffman et al., 2020).
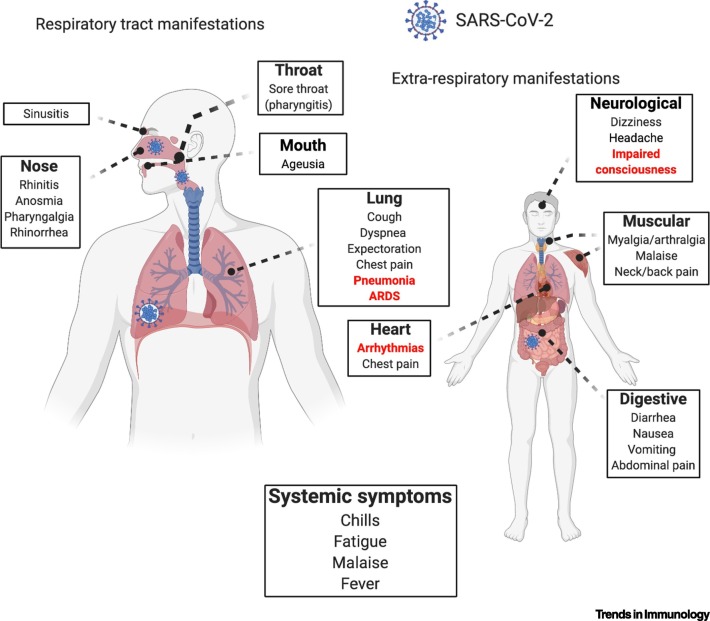
Figure 5. Systemic SARS-CoV-2 Infection. Failure to clear the virus may lead to infection of a wide range of extrapulmonary tissue such as the kidneys, heart, and intestines. Disease progression is accompanied by symptoms pertaining to the range of tissues affected (Harrison et al., 2020)
Advanced Infection & Multi-Organ Tropism
Upon replication and release of viral particles in the lungs, symptoms such as cough, fever, and muscle pain begin to present themselves. These symptoms present approximately 6 days after initial infection. At this point in the infection cycle, many patients may clear the infection in an additional 4-5 days (Guan et al., 2020). If the infection is not successfully cleared during this stage, it may proceed to more severe presentation characterized by multi-organ tropism, severe inflammation, and multi-organ dysfunction. At around 7 to 14 days after initial exposure, the virus may gain access to, and be proliferated via, the bloodstream (viremia) (Guan et al., 2020). Upon the commencement of this stage of infection, the virus may infect a number of body sites, such as the kidneys, intestines, and heart. Pulmonary complications, such as hypoxemia and shortness of breath, develop during this stage alongside complications in other infected organs (Wu et al., 2020). Examples include proteinuria and renal failure resulting from damage to the kidneys, arrhythmia, chest pain and cardiac failure resulting from infection of the heart, and nausea, abdominal pain and diarrhea resulting from enteric infection (Xiao et al., 2020) (Wu et al., 2020). The spread of SARS-CoV-2 to other tissue is largely dependent on presentation of ACE2 and other target cell surface proteins in these sites. For instance, enteric infections are common across viremic COVID-19 patients due to high expression of ACE2 and TMPRSS2 in the brush border of enterocytes (Xiao et al., 2020). COVID-19 samples have been recovered from stool samples recovered from 20% of a cohort of patients studied by Xiao et al. (2020), strongly suggesting a fecal-oral transmission route.
Immunopathology
As with other viral infections, SARS-CoV-2 infection can trigger activation of innate and adaptive immune responses that can be both beneficial and detrimental to limiting pathogenicity. While such responses are a fundamental mechanism underlying vaccination, if under- or over-stimulated they may serve to worsen the health of the patient. Rampant, dysregulated innate inflammatory responses and muted adaptive responses may lead to local and systemic tissue damage. Lymphopenia is a hallmark feature of severe presentations of COVID-19, characterized by drastically reduced numbers of CD4+ T cells, CD8+ T cells, B cells, and NK (natural killer) cells. Additionally, COVID-19 patients display upregulated NKG2A exhaustion markers on NK cells and CD8+ T cells (Qin et al., 2020). These cells are exhausted, or functionally paralyzed, due to overactivation. Such a mechanism ordinarily serves to attenuate immune function but correlates with increased inflammation and worsened clinical outcomes in COVID-19 patients (Zhou et al., 2020). This diminishment of adaptive immune agents is accompanied by a similarly disproportionate increase in neutrophil count. In addition, patients display what is known as a cytokine storm, characterized by a rapid and drastic increase in pro-inflammatory cytokines such as IL-6, IL-1β, IL-2, IL-8, and IL-17 (Qin et al., 2020). The release of innate cytokines can lead to activation of naïve CD4+ helper T cells, which, in turn, contribute to activation and differentiation of B cells which, in turn, release cytokines (Zhou et al., 2020). This results in a feedback loop where cytokines induce activation of CD4+ T cells, which induces greater cytokine activation, which, in turn, activates more CD4+ T cells. This feedback loop contributes to the cytokine storm seen in severe manifestations of COVID-19, resulting in an uncontrolled inflammatory response that causes local and systemic tissue damage, indicates high disease severity, and precipitates poor clinical outcomes (Qin et al., 2020) (Xu et al., 2020). Much of the organ damage and failure that is typical of severe COVID-19, such as acute respiratory distress syndrome (ARDS), cardiac failure or kidney failure, is caused by these runaway systemic responses (Qin et al., 2020).
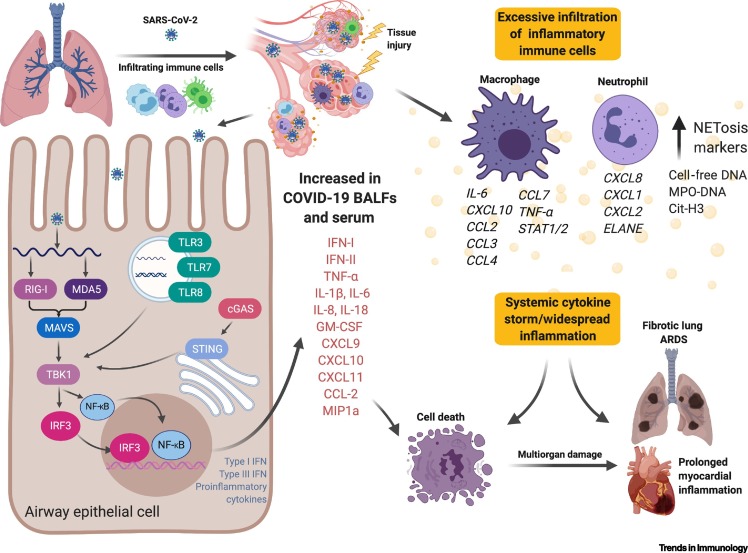
Figure 6. Lung Inflammation and Immunopathology Following SARS-CoV-2 Infection. Upon inhalation of SARS-CoV-2 viral particles, an innate inflammatory response is triggered following detection by immune sensors, such as Toll-like Receptors (TLRs). This mediates tissue damage and fibrosis in the lungs, leading to cell death. These inflammatory immunopathologies are mirrored in other tropisms, such as the heart (Harrison et al., 2020)
Despite the fact that SARS-CoV-2 infiltrates a number of tissue types, pulmonary damage has been best characterized. Most COVID-19 deaths occur as a result of respiratory complications owing to pneumonia or ARDS. This occurs due to detection of SARS-CoV-2 by innate immune sensors in the lower lung and the initiation of hyper-inflammatory response that breaks down vascular endothelium and alveolar epithelium. This causes flooding of interstitial fluid and protein into the alveoli and greatly diminishes gas exchange. Fibroblast-induced scar tissue formation following damage also reduces surface area for gas exchange via permanent pulmonary fibrosis (Harrison et al., 2020). These conditions eventually give rise to the most lethal respiratory sequelae of SARS-CoV-2 infection.
Clinical Presentation & Risk Factors
Clinical Presentation
Clinical symptoms would vary depending on the severity of the disease and in some cases, the variants of concern as well. The symptoms of SARS-CoV-2 can begin to show anywhere from 2-14 days post-infection (Mayo Clinic, 2022). Most patients will show signs of COVID-19 about 11.5 days post-infection (Cascella et al., 2022). Some symptoms are listed as the following (Mayo Clinic, 2022):
- Fever
- Runny nose
- Headaches
- Cough, sore throat
- Tiredness
- Chills
- Diarrhea, vomiting, nausea
- Anosmia
There are different types of disease progression, which can be categorized as the following: asymptomatic or pre-symptomatic infection, mild illness, moderate illness, severe illness, and critical illness (Cascella et al., 2022).
- Asymptomatic or pre-symptomatic infection - Individuals are infected with the disease but do not have symptoms associated with the disease (Cascella et al., 2022).
- Mild illness - Individuals are infected and have symptoms of the disease (Cascella et al., 2022).
- Moderate illness - Individuals who are infected, and upon further tests, have lower respiratory tract disease and SpO2 of greater than or equal to 94% (Cascella et al., 2022).
- Severe illness - Individuals who are infected and have an SpO2 less than or equal to 94%, a PaO2/FiO2 of less than 300 (Cascella et al., 2022).
- Critical illness - Individuals are infected and experience acute respiratory failure and organ failure, as well as septic shock. Often characterized by ventilation, either non-invasive or mechanical (Cascella et al., 2022).
When conducting laboratory tests to determine clinicopathological components of the disease, studies found elevated levels of C-reactive proteins, cardiac enzymes, D-dimer, erythrocyte sedimentation rate, and procalcitonin (Cascella et al., 2022). Abnormalities in liver and renal function were also reported (Cascella et al., 2022).
Clinical presentation can also vary by the variant of disease. Some variants can cause higher incidence of serious disease. Multiple studies have found that the B.1.1.7 variant, also known as the Alpha variant, shows increased counts of severe disease compared to the original strain (Cascella et al., 2022). At first, no significant increase in hospitalization or mortality rates were associated with the Alpha variant. However, subsequent studies have shown a higher risk of mortality among individuals with the Alpha variant compared to the original strain (Cascella et al., 2022). The B.1.351 variant, also known as the Beta variant, is found to increase transmission and reduce effectiveness against COVID-19 therapies such as monoclonal antibody therapy (Cascella et al., 2022). The P.1 variant, more commonly referred to as the Gamma variant, has also been found to reduce effectiveness of COVID-19 therapies as well (Cascella et al., 2022). The B.1.617.2 variant, also known as the Delta variant, was found to be highly infectious, about two times more compared to previous variants, increasing hospitalization and mortality rates (Katella, 2022). The fifth variant of concern, B.1.1.529, also known as Omicron, suggests through modelling that it is highly infectious, about 2.8 times more infectious than the Delta variant (Cascella et al., 2022). It also reduces effectiveness against COVID-19 therapies such as monoclonal antibodies, but other therapies are still deemed effective against the variant (Cascella et al., 2022).
Risk Factors
Some risk factors which increase the severity of disease from COVID-19 are listed as the following (Mayo Clinic, 2022):
- Heart diseases
- Immunocompromised individuals
- Diabetes
- High blood pressure
- Liver, lung, and kidney disease
- Individuals who use and abuse substances
- Pregnancy
- Asthma
- Cancer
Interestingly, COVID-19 symptoms vary according to different risk factors. Individuals with the risk factors mentioned before display higher incidence of moderate to severe disease (Mayo Clinic, 2022). Age also plays a factor in determining disease severity (Mayo Clinic, 2022). For example, children display minor symptoms and mild disease, compared to middle-aged and elderly individuals that are at higher risk of developing serious disease (Mayo Clinic, 2022). The patients at highest risk for severe disease are individuals that are 60 years and older with various medical conditions (Cascella et al., 2022). Of these individuals, male infected patients were more likely to develop severe disease and succumb to SARS-CoV-2 compared to female infected patients (Cascella et al., 2022). Other risk factors which can spread disease are being in close contact with an infected individual (less than 6 feet), and inhaling or being in contact with infected droplets after an infected individual sneezes or coughs (Mayo Clinic, 2022). One also needs to address the social circumstances of an individual and the potential for them to develop severe disease. Unfortunately, racial and ethnic disparities play a part in determining disease progression and mortality rates (Cascella et al., 2022). Racialized individuals, as well as those from ethnic minorities, are exposed to COVID-19 at a higher level compared to White individuals (Cascella et al., 2022). This is often due to certain racial and ethnic groups being less financially well-off, leading to poorer health outcomes due to lack of access to nutritious foods (Ro, 2020). This leads to individuals developing underlying conditions and medical comorbidities which become a risk factor for contracting severe SARS-CoV-2 disease (Ro, 2020). As well, many racialized and ethnic minorities work difficult, hazardous jobs with long hours and low pay. As a result, they often have to work multiple jobs to sustain themselves and their families, leading to increased exposure. Lockdowns also are unfavorable against certain groups as it leads to loss of income, translating to poorer health outcomes, compared to upper class individuals who are fortunate enough to have the financial resources to last through lockdowns (Ro, 2020). Finally, certain racial and ethnic groups often live in environments which pose a risk factor for severe disease. These environments are often polluted, where the air quality is lower compared to certain residential areas. These include housing near industrial areas, highways, and landfill sites (Ro, 2020). Due to the poorer air quality, this often triggers respiratory irritation and conditions which leads to an increase in severe disease and mortality rates due to increased vulnerability to respiratory tract diseases like COVID-19 (Ro, 2020).
Transmission
The transmission of COVID-19 refers to the passing of the virus from one infected person, whether symptomatic or asymptomatic, to another individual. Transmission of this virus occurs more rapidly when infected individuals are in close contact with uninfected individuals, however, the virus can become airborne and infection can occur over longer distances. The SARS-CoV-2 virus follows a horizontal mode of transmission, meaning the virus spreads from person to person. Contrasting this is a vertical mode of transmission where a mother passes the virus to her offspring, however vertical transmission of COVID-19 is extremely rare (Fornari 2020). Transmission may occur directly from person-to-person or can occur after viral particles are deposited on surfaces outside host bodies. As such, important factors dictating transmission are qualities such as doubling rate. Doubling rate of SARS-CoV-2 viral particles have been shown to range from 2 to 5 days, mitigated by adherence to sanitation guidelines (Cevik et al., 2021).
Infectious Period
Once an individual has become infected, it may take up to fourteen days before symptom onset. This period is known as the incubation period, and individuals who have contracted COVID-19 may transmit it during this period as well as after the onset of symptoms (Ferretti et. al. 2020)(Pollock & Lancaster 2020). During the incubation period, the virus is entering host cells and utilizing the host machinery to replicate their RNA. The virus is then able to synthesize infectious virions which replicate and infect more host cells. Once the virus is recognized by the immune system, the immune response will occur to aid in clearing the infection. This is when the onset of symptoms occurs for most individuals and may take up to fourteen days (Ferretti et. al. 2020). The viral load is highest once symptom onset occurs and therefore an individual is the most infectious during this time. The viral load is a numerical expression that refers to the quantity of a given virus in the body and the coincidence of its increase with symptom onset sets ideal conditions for greater transmission. However, by the same token, transmission from symptomatic individuals may be more easily curbed than the much more inconspicuous transmission that results from asymptomatic individuals.
Asymptomatic Transmission
While most individuals who contract COVID-19 begin to show symptoms several days after contracting the virus, there are a fraction of individuals who do not show any symptoms over the course of their infectious period. These individuals are known as asymptomatic carriers of COVID-19 and although they are not showing symptoms, they may still transmit the virus to uninfected individuals through various different modes of transmission (Pollock & Lancaster 2020). SARS-CoV-2 infection may also proceed through an early, presymptomatic period before the onset of symptoms. During this presymptomatic phase, lasting from 1-2 weeks, risk of transmission may be higher despite lower viral load due to a lack of appropriate isolation measures when illness is not readily apparent. For these reasons, it is difficult to track asymptomatic transmission rates as the sources of such are inherently inconspicuous (Cevik et al., 2021).
Common Modes of Transmission
Respiratory viruses can be transmitted via 3 main routes: contact transmission, droplet transmission, and airborne transmission (Lotfi et al., 2020). Contact transmission occurs when an individual comes into direct contact with an infected individual or touches a surface that has been contaminated with a virus. Droplet transmission of large and small respiratory droplets that contain a virus can occur when an individual is in close proximity to an infected person (Lotfi et al., 2020). And lastly, airborne transmission can occur via small droplets and particles that are suspended in the air over long distances and time, compared to droplet transmission (Lotfi et al., 2020).
The dominant mode of transmission of COVID-19 is exposure to respiratory droplets that carry the virus through airborne/aerosol transmission (Zhang et al., 2020). Respiratory droplets that contain the virus are released when an infected individual speaks, coughs, sneezes etc. When this occurs, viral shedding takes place to produce large droplets and small aerosols (Zhang et al., 2020). Large droplets settle out of the air and cause person/object contamination whereas the small aerosols become dispersed within the air (Zhang et al., 2020). Inhalation, ingestion or exposure of droplets to mucous membranes can subsequently lead to infection (Lotfi et al., 2020). Objects that indirectly propagate SARS-CoV-2 infection after exposure to droplets are called fomites. Individuals that come into contact with these objects may then themselves be infected, however, this can be curbed with adherence to sanitization procedures. Airborne transmission via aerosols can occur over both extended periods of time and distance and when inhaled, the virus deposits along the respiratory tract (Zhang et al., 2020). Droplets can only traverse roughly 6 feet after expulsion and only remain in the air for a limited period of time, but SARS-CoV-2 remains intact as well as contagious and can be suspended within the air for up to 3 hours in aerosols (Lotfi et al., 2020). With normal nasal breathing, the inhalation of airborne viruses leads to direction and continuous deposition into the human respiratory tract (Zhang et al., 2020). Fine aerosols are able to penetrate deeply into the respiratory tract and may be able to reach vital organs (Zhang et al., 2020). Due to their small size (< 5um), viral particles in aerosols can be retained in the surrounding air for up to 3 hours and have a half-life in airborne suspension comparable to fomites (approximately 1 hour). Deposited into the surrounding air through sneezing or coughing, aerosol transmission can be dependent on any number of factors such as weather, humidity, temperature and ventilation (van Doralemen et al., 2020).
Prevention of airborne transmission can be accomplished via the usage of masks, physical distancing, adequate ventilation and avoidance of crowded indoor spaces. Facial coverings are key to preventing airborne transmission as they block atomization and inhalation of virus-bearing aerosol and contact transmission by blocking viral shedding (Zhang et al., 2020).
Rare Modes of Transmission
Figure 7. SARS-CoV-2 transmission mechanisms. SARS-CoV-2 can be transmitted through respiratory droplets, aerosol dispersion, and more rarely, through fecal-oral transmission (Harrison et al., 2020)
Three less dominant modes of transmission of COVID-19 include transmission via surfaces, animal vectors and a fecal-oral route.
Although studies conducted have concluded that aerosolized SARS-CoV-2 remains viable within aerosols and on various surfaces for 4-72 hours, infection caused by this mode of transmission is low (Karia et al., 2020). However, infection can occur if an individual touches a surface that has been contaminated with SARS-CoV-2 and then comes into contact with a mucosal membrane such as the eyes, nose or mouth (Lotfi et al., 2020). Prevention of infection via these modes of transmission can be done by hand washing/sanitizing and periodic surface cleaning with disinfectant.
It is assumed that SARS-CoV-2 was initially transmitted from animals to humans, but the infection is sustained by human-to-human transmission (Tiwari et al., 2020). The risk of animals spreading SARS-CoV-2 to humans is low, but the virus can be spread from humans to animals during close contact (CDC, 2021). There have been reports of animals infected with SARS-CoV-2 following exposure to humans infected with COVID-19. Animals that have been reported to be infected include companion animals such as pet cats, dogs, and ferrets, zoo animals and animals living in sanctuaries such as otters, non-human primates, and hyenas, mink on farmland as well as wild white-tailed deer (CDC, 2021).
It has also been reported that there may be possible fecal-oral transmission of SARS-CoV-2 (Harrison et al., 2020). Gastrointestinal illness has been reported in patients infected with COVID-19 which is consistent with the recovery of SARS-CoV from fecal samples of 30% of patients infected with SARS-CoV in a cohort study (Harrison et al., 2020). This route is plausible as RNA-loaded aerosols were found near toilet bowls as well as detectable SARS-CoV-2 RNA from rectal swabs (Harrison et al., 2020).
Conclusion & Future Steps
A fundamental characteristic of severe COVID-19 disease presentation is its ability to migrate from pulmonary tissue to targets such as the heart, kidney and intestines. Further into the mechanisms by which SARS-CoV-2 migrates and bypasses physiological filtration barriers is necessary. Additionally, it will be prudent to understand if the binding mechanism employed to target non-pulmonary tissue differs in any way from pulmonary targets, such as through the presence of cognate cell surface receptors other than ACE2.
Other innate cell characteristics have been identified in mediating SARS-CoV-2 infection. As such, the possibility that the same is true for non-respiratory cellular targets must be investigated further. Since multiple organ failure is a prominent cause of death for COVID-19 patients, research into these areas has several potential therapeutic applications.
Another area of further study pertaining to SARS-CoV-2 pathogenesis relates to the mechanisms of cell infiltration and viral replication. The viral genome encodes nine accessory proteins that have, so far, not been as well characterized as the structural proteins. Understanding how, or if, these proteins regulate SARS-CoV-2 infection and their mechanisms of action may serve as the basis for the development and enhancement of COVID-19 drug development.
Finally, the emergence of a wide variety of SARS-CoV-2 strains and mutants will necessitate keen vigilance on how what is currently understood about the virus may change as they pertain to pathogenesis and transmission.
Presentation Slides
References
A timeline of covid-19 vaccine developments in 2021. AJMC. (n.d.). Retrieved January 27, 2022, from https://www.ajmc.com/view/a-timeline-of-covid-19-vaccine-developments-in-2021
BPS. (n.d.). SARS-COV-2 variants. SARS-Cov-2 Variants. Retrieved February 3, 2022, from https://bpsbioscience.com/sars-cov-2-variants
Cable News Network (CNN). (2022, January 5). Covid-19 pandemic timeline fast facts. CNN. Retrieved January 27, 2022, from https://www.cnn.com/2021/08/09/health/covid-19-pandemic-timeline-fast-facts/index.html
Cascella, M., Rajnik, M., Cuomo, A., Dulebohn, S. C., & Di Napoli, R. (2022). Features, Evaluation, and Treatment of Coronavirus (COVID-19). StatPearls. https://www.ncbi.nlm.nih.gov/books/NBK554776/
Centers for Disease Control and Prevention (CDC). (n.d.). About Middle East respiratory syndrome (MERS). Centers for Disease Control and Prevention. Retrieved January 27, 2022, from https://www.cdc.gov/coronavirus/mers/about/index.html
Cevik, M., Tate, M., Lloyd, O., Maraolo, A. E., Schafers, J., & Ho, A. (2021). SARS-COV-2, SARS-COV, and MERS-COV viral load dynamics, duration of viral shedding, and infectiousness: A systematic review and meta-analysis. The Lancet Microbe, 2(1). https://doi.org/10.1016/s2666-5247(20)30172-5
Coronavirus disease 2019 (COVID-19) - Symptoms and causes - Mayo Clinic. (n.d.). Retrieved January 23, 2022, from https://www.mayoclinic.org/diseases-conditions/coronavirus/symptoms-causes/syc-20479963
Coronavirus: Why some racial groups are more vulnerable - BBC Future. (n.d.). Retrieved January 23, 2022, from https://www.bbc.com/future/article/20200420-coronavirus-why-some-racial-groups-are-more-vulnerable
Ehre, C. (2020). SARS-COV-2 infection of airway cells. New England Journal of Medicine, 383(10), 969–969. https://doi.org/10.1056/nejmicm2023328
Ferretti, L., Ledda, A., Wymant, C., Zhao, L., Ledda, V., Abeler-Dörner, L., Kendall, M., Nurtay, A., Cheng, H.-Y., Ng, T.-C., Lin, H.-H., Hinch, R., Masel, J., Kilpatrick, A.
M., & Fraser, C. (2020). The timing of COVID-19 transmission. https://doi.org/10.1101/2020.09.04.20188516
Fornari, F. (2020). Vertical transmission of COVID-19-A systematic review. Journal of Pediatrics, Perinatology and Child Health, 04(02). https://doi.org/10.26502/jppch.74050034
Harrison, A. G., Lin, T., & Wang, P. (2020). Mechanisms of SARS-COV-2 transmission and pathogenesis. Trends in Immunology, 41(12), 1100–1115. https://doi.org/10.1016/j.it.2020.10.004
Health Canada (2022, January 7). Government of Canada. COVID-19 Vaccines: Authorized vaccines - Canada.ca. Retrieved January 27, 2022, from https://www.canada.ca/en/health-canada/services/drugs-health-products/covid19-industry/drugs-vaccines-treatments/vaccines.html
Hoffmann, M., Kleine-Weber, H., & Pöhlmann, S. (2020). A multibasic cleavage site in the spike protein of SARS-COV-2 is essential for infection of human lung cells. Molecular Cell, 78(4). https://doi.org/10.1016/j.molcel.2020.04.022
Hoffmann, M., Kleine-Weber, H., Schroeder, S., Krüger, N., Herrler, T., Erichsen, S., Schiergens, T. S., Herrler, G., Wu, N.-H., Nitsche, A., Müller, M. A., Drosten, C., & Pöhlmann, S. (2020). SARS-COV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell, 181(2). https://doi.org/10.1016/j.cell.2020.02.052
Huang, Y., Yang, C., Xu, X.-feng, Xu, W., & Liu, S.-wen. (2020). Structural and functional properties of SARS-COV-2 spike protein: Potential antivirus drug development for covid-19. Acta Pharmacologica Sinica, 41(9), 1141–1149. https://doi.org/10.1038/s41401-020-0485-4
Jackson, C. B., Farzan, M., Chen, B., & Choe, H. (2021). Mechanisms of SARS-COV-2 entry into cells. Nature Reviews Molecular Cell Biology, 23(1), 3–20. https://doi.org/10.1038/s41580-021-00418-x
Karia, R., Gupta, I., Khandait, H., Yadav, A., & Yadav, A. (2020). Covid-19 and its modes of transmission. SN Comprehensive Clinical Medicine, 2(10), 1798–1801. https://doi.org/10.1007/s42399-020-00498-4
Lotfi, M., Hamblin, M. R., & Rezaei, N. (2020). Covid-19: Transmission, prevention, and potential therapeutic opportunities. Clinica Chimica Acta, 508, 254–266. https://doi.org/10.1016/j.cca.2020.05.044
Lu, R., Zhao, X., Li, J., Niu, P., Yang, B., Wu, H., Wang, W., Song, H., Huang, B., Zhu, N., Bi, Y., Ma, X., Zhan, F., Wang, L., Hu, T., Zhou, H., Hu, Z., Zhou, W., Zhao, L., … Tan, W. (2020). Genomic characterisation and epidemiology of 2019 novel coronavirus: Implications for virus origins and receptor binding. The Lancet, 395(10224), 565–574. https://doi.org/10.1016/s0140-6736(20)30251-8
Pollock, A. M., & Lancaster, J. (2020). Asymptomatic transmission of covid-19. BMJ, m4851. https://doi.org/10.1136/bmj.m4851
Qin, C., Zhou, L., Hu, Z., Zhang, S., Yang, S., Tao, Y., Xie, C., Ma, K., Shang, K., Wang, W., & Tian, D.-S. (2020). Dysregulation of immune response in patients with coronavirus 2019 (COVID-19) in Wuhan, China. Clinical Infectious Diseases, 71(15), 762–768. https://doi.org/10.1093/cid/ciaa248
Shulla, A., Heald-Sargent, T., Subramanya, G., Zhao, J., Perlman, S., & Gallagher, T. (2011). A transmembrane serine protease is linked to the severe acute respiratory syndrome coronavirus receptor and activates virus entry. Journal of virology. Retrieved January 27, 2022, from https://pubmed.ncbi.nlm.nih.gov/21068237/
The Lancet Respiratory Medicine. (2020). Covid-19 transmission—up in the Air. The Lancet Respiratory Medicine, 8(12), 1159. https://doi.org/10.1016/s2213-2600(20)30514-2
van Doremalen, N., Bushmaker, T., Morris, D. H., Holbrook, M. G., Gamble, A., Williamson, B. N., Tamin, A., Harcourt, J. L., Thornburg, N. J., Gerber, S. I., Lloyd-Smith, J. O., de Wit, E., & Munster, V. J. (2020). Aerosol and surface stability of SARS-COV-2 as compared with SARS-COV-1. New England Journal of Medicine, 382(16), 1564–1567. https://doi.org/10.1056/nejmc2004973
V’kovski, P., Kratzel, A., Steiner, S., Stalder, H., & Thiel, V. (2020). Coronavirus Biology and replication: Implications for SARS-COV-2. Nature Reviews Microbiology, 19(3), 155–170. https://doi.org/10.1038/s41579-020-00468-6
World Health Organization. (n.d.). Coronavirus disease (covid-19). World Health Organization. Retrieved January 27, 2022, from https://www.who.int/emergencies/diseases/novel-coronavirus-2019
World Health Organization. (n.d.). Middle East respiratory syndrome coronavirus (MERS-COV). World Health Organization. Retrieved January 27, 2022, from https://www.who.int/health-topics/middle-east-respiratory-syndrome-coronavirus-mers#tab=tab_2
World Health Organization. (n.d.). Severe acute respiratory syndrome (SARS). World Health Organization. Retrieved January 27, 2022, from https://www.who.int/health-topics/severe-acute-respiratory-syndrome#tab=tab_3
World Health Organization. (n.d.). Tracking sars-COV-2 variants. World Health Organization. Retrieved January 27, 2022, from https://www.who.int/en/activities/tracking-SARS-CoV-2-variants/
Wu, H.-Y., & Brian, D. A. (2010). Subgenomic messenger RNA amplification in Coronaviruses. Proceedings of the National Academy of Sciences, 107(27), 12257–12262. https://doi.org/10.1073/pnas.1000378107
Wu, L., O'Kane, A. M., Peng, H., Bi, Y., Motriuk-Smith, D., & Ren, J. (2020). SARS-COV-2 and cardiovascular complications: From molecular mechanisms to pharmaceutical management. Biochemical Pharmacology, 178, 114114. https://doi.org/10.1016/j.bcp.2020.114114
Xiao, F., Tang, M., Zheng, X., Liu, Y., Li, X., & Shan, H. (2020). Evidence for gastrointestinal infection of SARS-COV-2. Gastroenterology, 158(6). https://doi.org/10.1053/j.gastro.2020.02.055
Zhang, Y.-Z., & Holmes, E. C. (2020). A genomic perspective on the origin and emergence of SARS-COV-2. Cell, 181(2), 223–227. https://doi.org/10.1016/j.cell.2020.03.035
Zhao, Y., Zhao, Z., Wang, Y., Zhou, Y., Ma, Y., & Zuo, W. (2020). Single-cell RNA expression profiling of ACE2, the receptor of SARS-COV-2. American Journal of Respiratory and Critical Care Medicine, 202(5), 756–759. https://doi.org/10.1164/rccm.202001-0179le
Zhou, Y., Fu, B., Zheng, X., Wang, D., Zhao, C., qi, Y., Sun, R., Tian, Z., Xu, X., & Wei, H. (2020). Aberrant pathogenic GM-CSF+ T cells and inflammatory CD14+CD16+ monocytes in severe pulmonary syndrome patients of a new coronavirus. https://doi.org/10.1101/2020.02.12.945576
Zhou, P., Yang, X.-L., Wang, X.-G., Hu, B., Zhang, L., Zhang, W., Si, H.-R., Zhu, Y., Li, B., Huang, C.-L., Chen, H.-D., Chen, J., Luo, Y., Guo, H., Jiang, R.-D., Liu, M.-Q., Chen, Y., Shen, X.-R., Wang, X., … Shi, Z.-L. (2020). A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature, 579(7798), 270–273. https://doi.org/10.1038/s41586-020-2012-7
5 Things To Know About the Delta Variant > News > Yale Medicine. (n.d.). Retrieved January 23, 2022, from https://www.yalemedicine.org/news/5-things-to-know-delta-variant-covid